It is important that lines 1 and 2 are traced to the superior aspect of the odontoid peg:

C1 - C4 = 4-7mm (should "hug" the anterior cortex)
C5 - C7 = 16-20mm (roughly equal to the vertebral body)

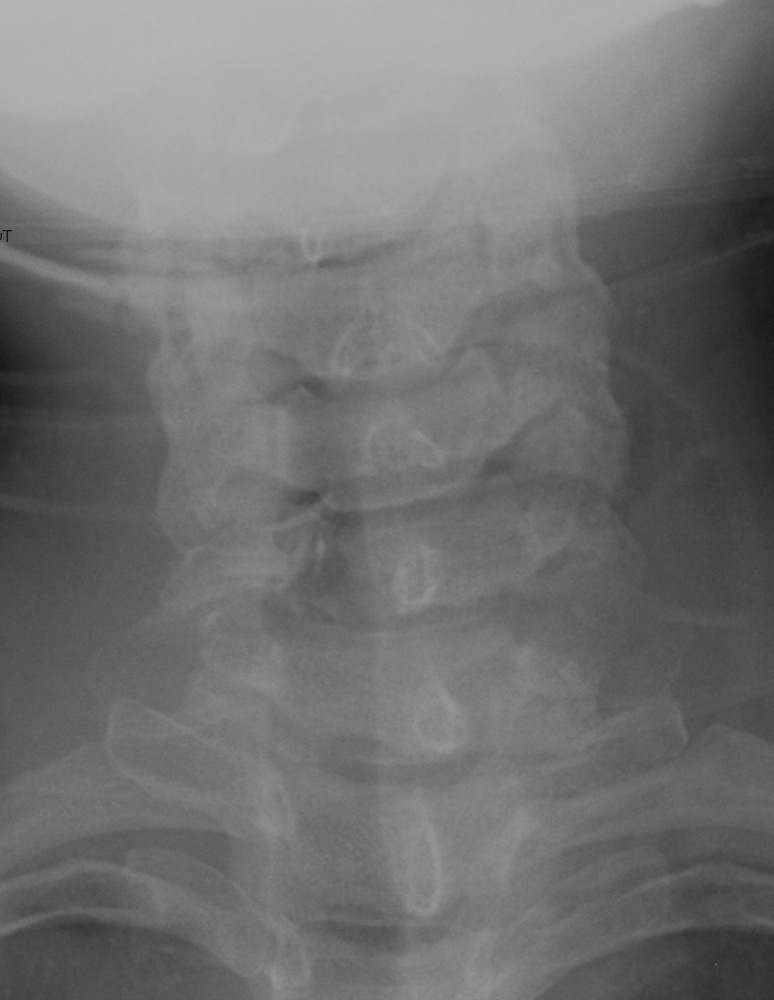






Intervertebral foramina, and the presence of osteophyte encroachment in spondylosis (OA).
Facet joints.
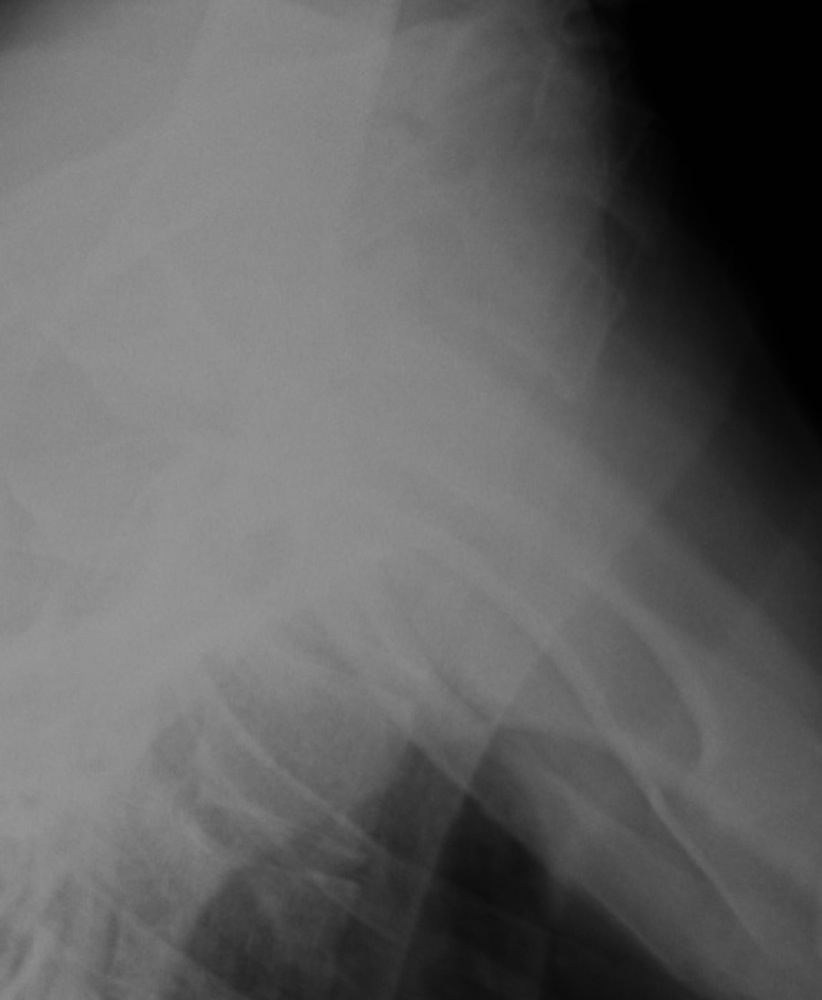
Alignment of C7 with T1 if the swimmer's view is unobtainable (30% obliques satisfactory).






This is a taut, strong structure that is closely applied to the anterior aspects of the vertebral bodies and the annulus of the intervertebral discs.
This is weaker, and is attached to the posterior vertebral bodies and intervertebral discs.
This ligament lines the dorsal surface of the spinal canal and is tightly applied to the laminae.
These interconnect the spinous processes.
Is applied to the dorsal tip of the spinous processes, and overlies the interspinous ligaments.
This is a longitudinal fracture through the posterior neural arch, usually bilateral. It is caused by hyperextension, with the result that the neural arch of C1 is compressed between the occiput and C2. It is best demonstrated on the lateral projection:
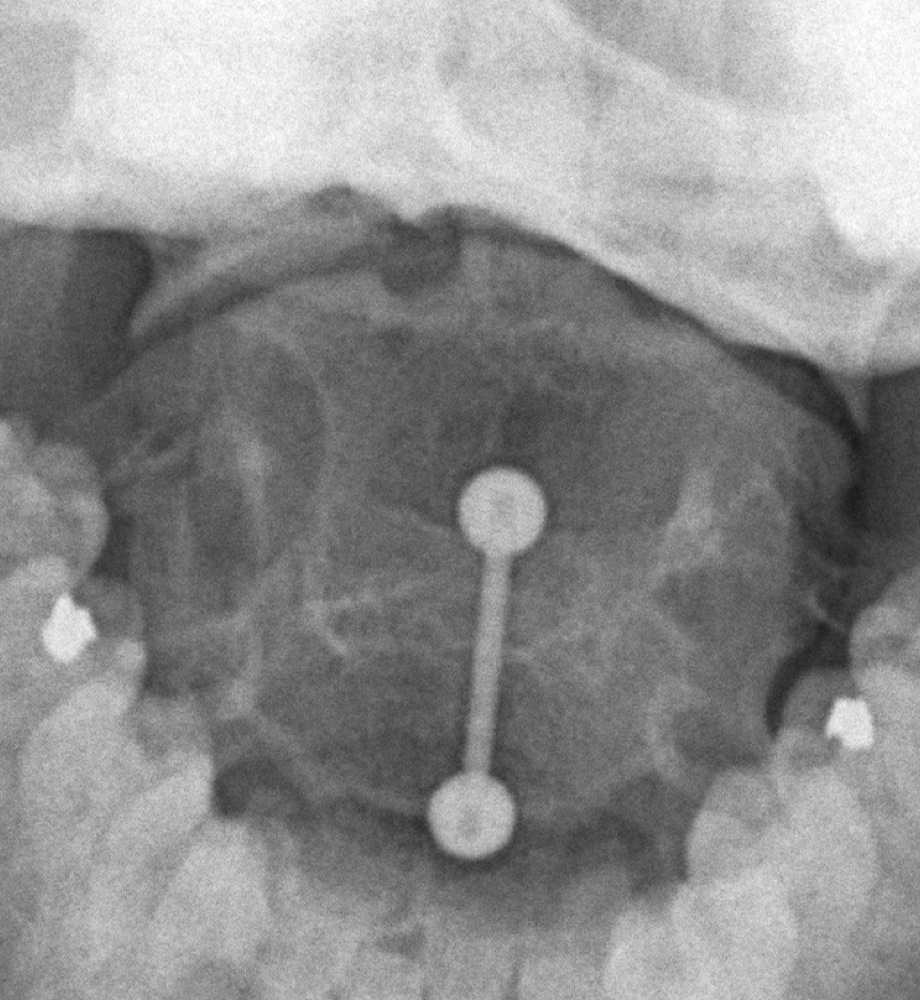
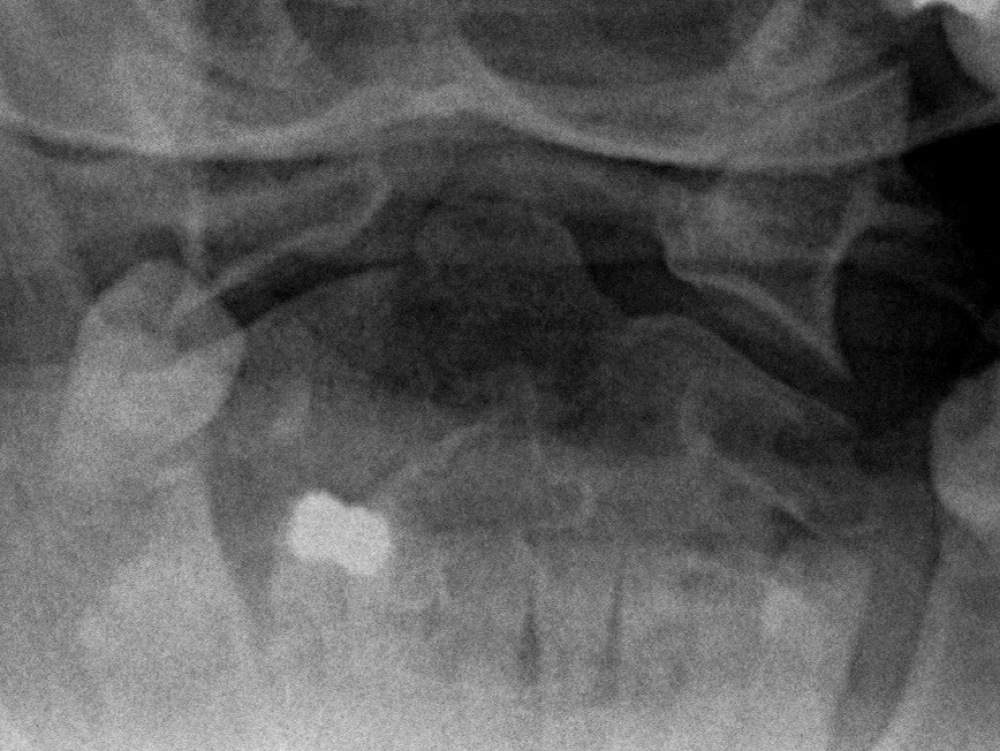
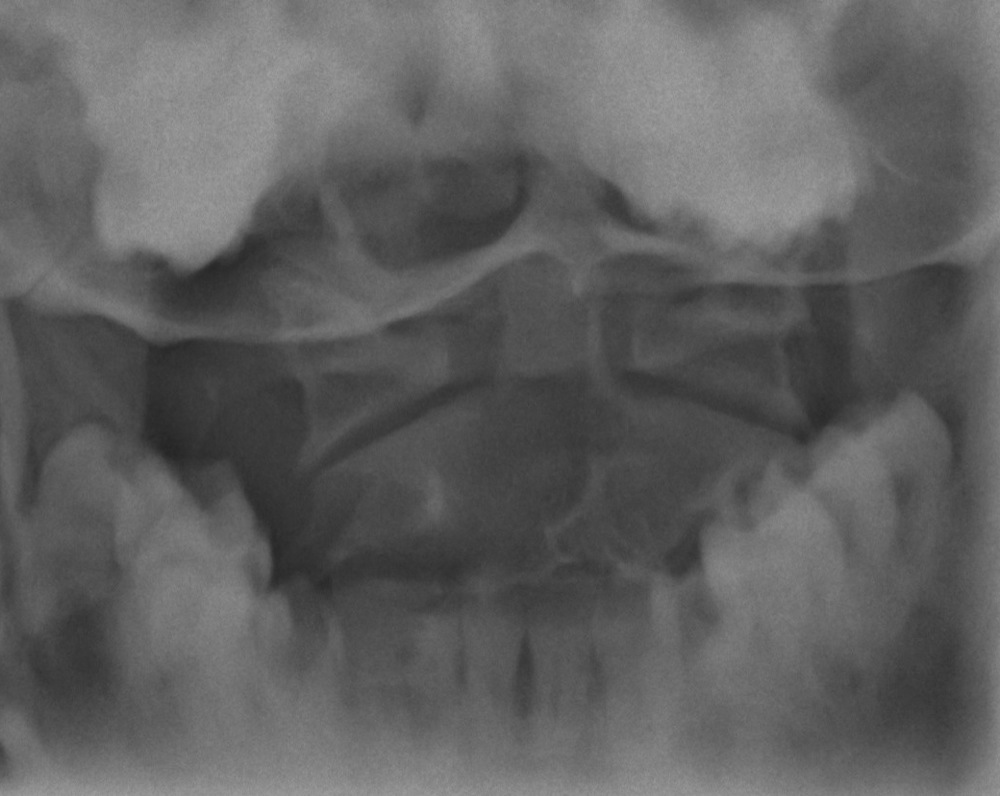
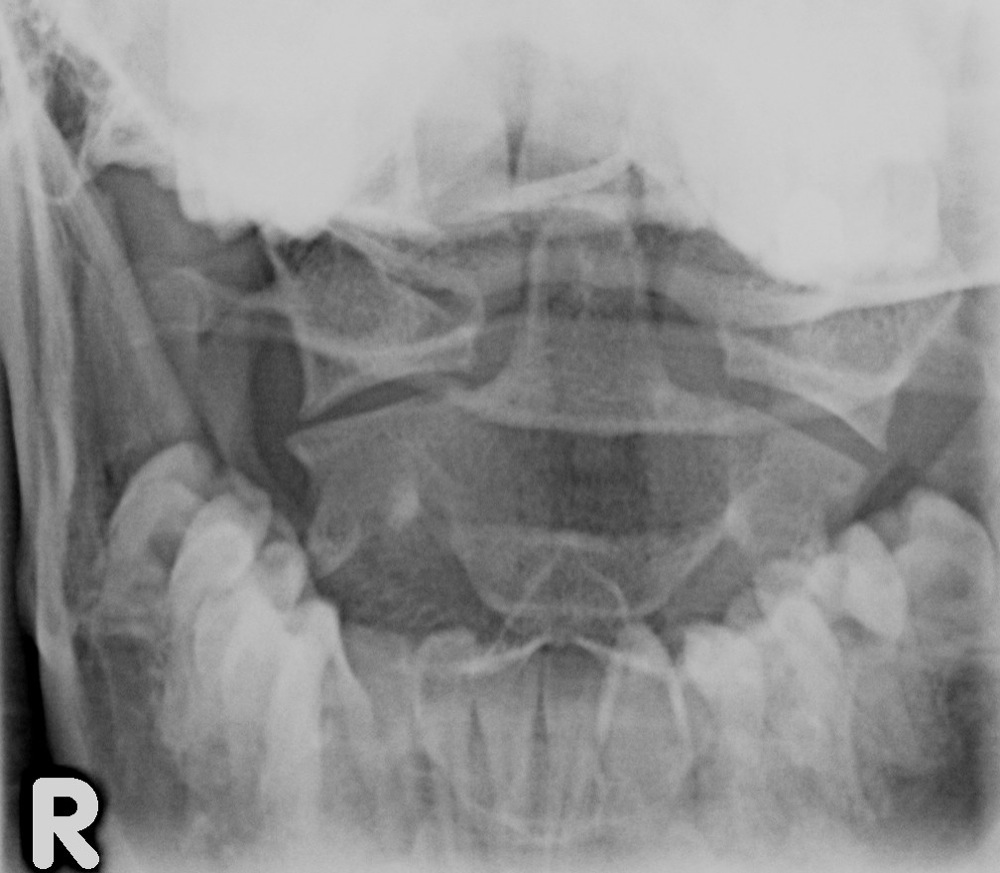
This is a comminuted fracture, with bilateral disruption of both anterior and posterior arches, and lateral displacement of both lateral masses. It is caused by axial compression with the transmission of force from the skull downwards through the occipital condyles, compressing the lateral masses. Demonstrated on the open mouth view by:
The injury is considered stable if the overhang is less than 7mm. Over 7mm indicates that the transverse ligament is disrupted, and is therefore unstable:
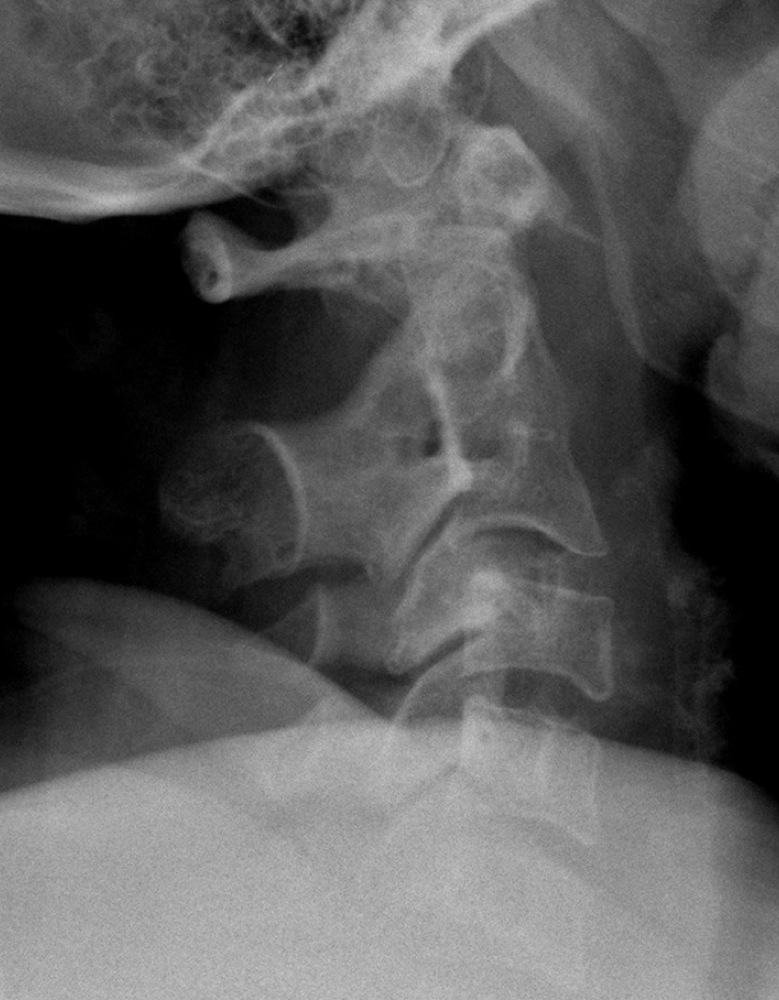
This is the most common fracture of C2. May be caused by flexion or extension and usually results in ligamentous instability. It usually involves the base of the peg and may be visualised on either the open mouth or, more commonly, lateral view. Assess for any soft tissue swelling anteriorly. Also look carefully at Harris' ring on the lateral projection:

Hyperextension of the neck transmits the force through to the C2 pedicles. This results in an oblique fracture originating anterior to the inferior facet of C2 and extending supero-posteriorly. Tension causes disruption of the anterior longitudinal ligament causing this injury to be unstable. Will be demonstrated on the lateral view but may be undisplaced:

This type of fracture is caused by hyperflexion with the result that the vertical height of the vertebral body is decreased anteriorly, as viewed on the lateral radiograph. The posterior elements remain intact. This is a stable injury:
Caused by axial compression, the intervertebral disc is driven into the vertebral body below. The vertebral body explodes into several fragments; a fragment from the postero-superior surface being driven posteriorly into the spinal canal. This is an unstable injury that frequently results in spinal cord injury. It is therefore important to check the posterior vertebral cortex for evidence of disruption, on an apparently simple wedge compression injury.
Flexion, rotation and distraction may cause the facet joints on one side to be locked. This results in the vertebra being displaced anteriorly by 25%, as demonstrated on the lateral radiograph. The facet joints are seen in true lateral profile above and oblique profile below, or vice versa:

Hyperextension causes a triangular fragment to be avulsed off the antero-inferior corner of the vertebral body. This is not associated with any neurological damage. The axis is most commonly involved:

This is an avulsion by the supraspinatous ligament off the spinous process, usually C6 or C7. This is caused by flexion as the body rotates relative to the head and neck. Usually undisplaced and therefore only seen on the lateral radiograph:

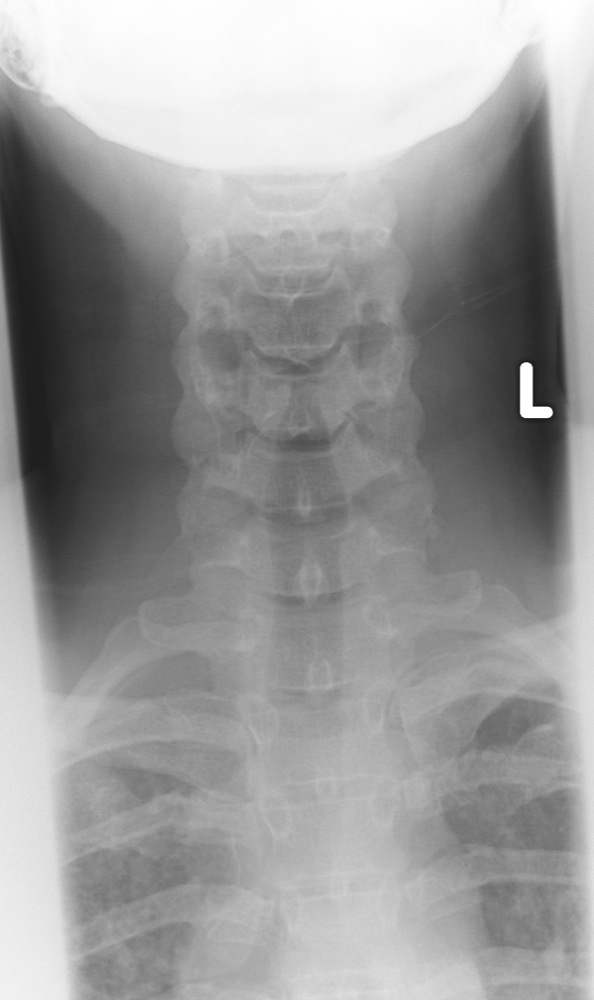
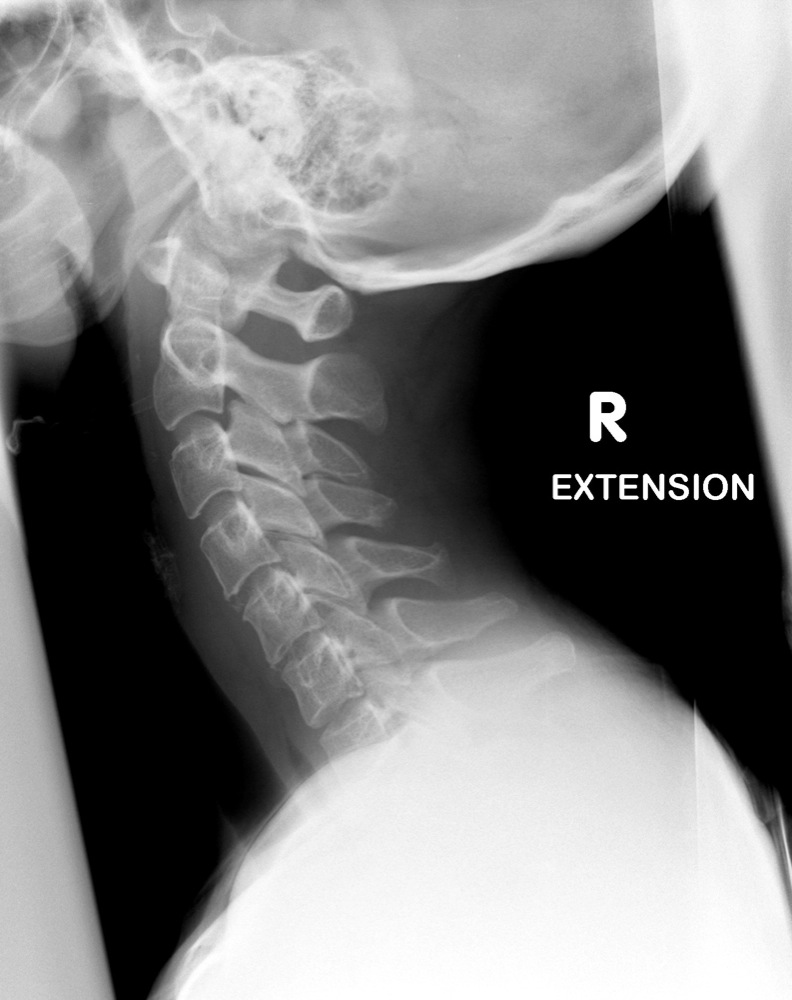
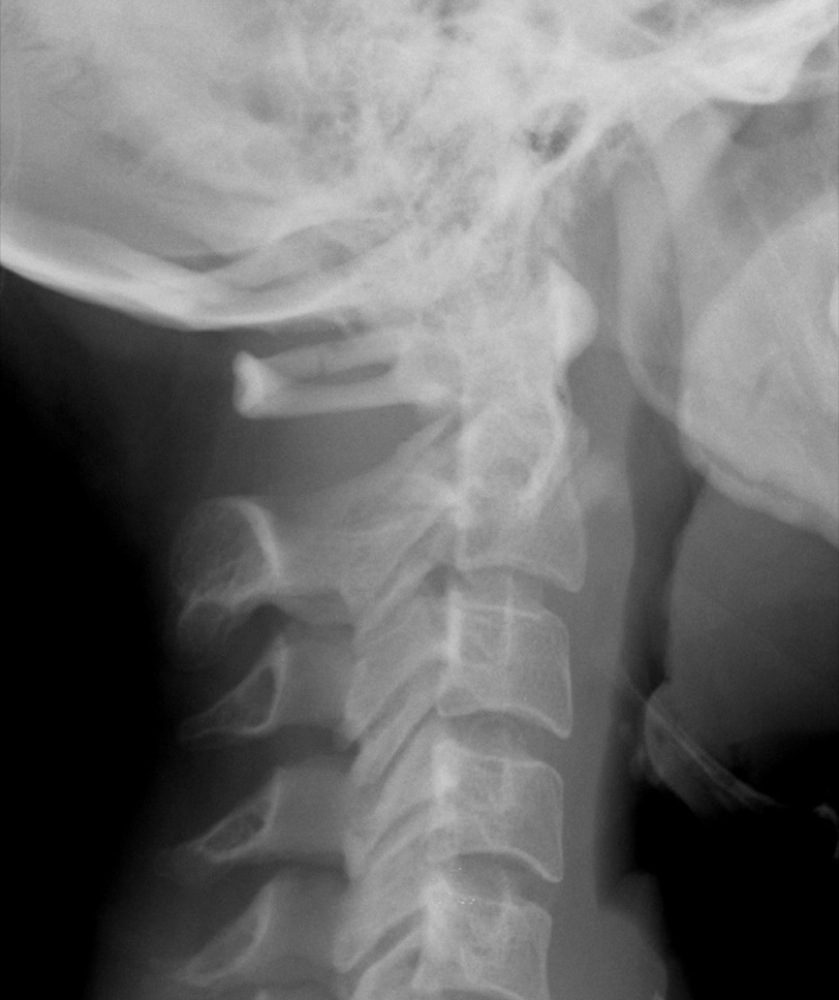
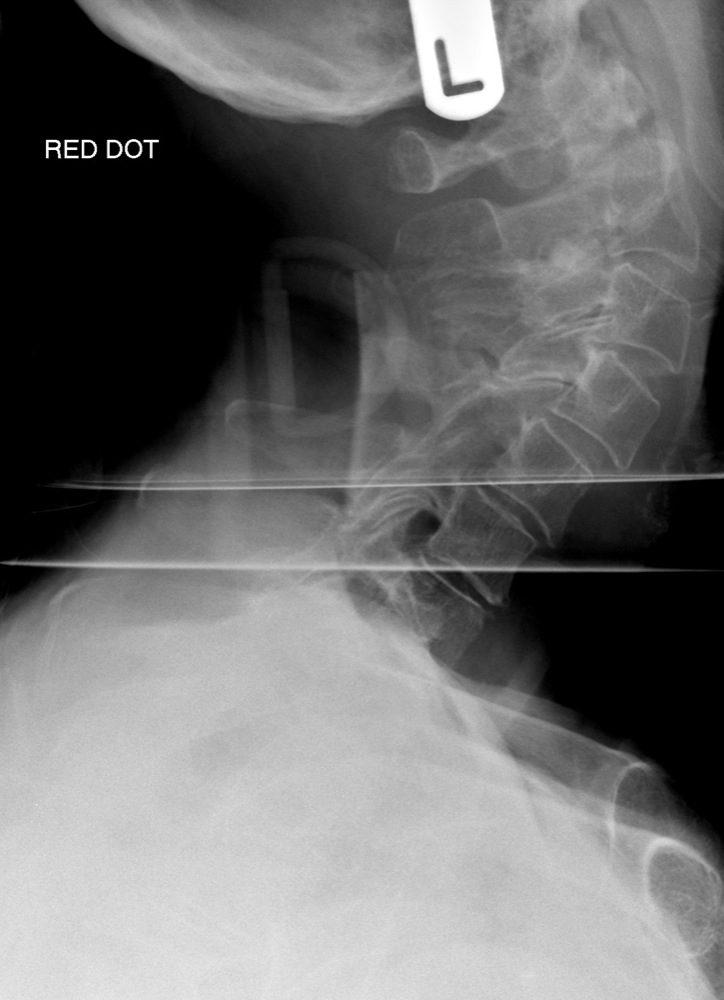
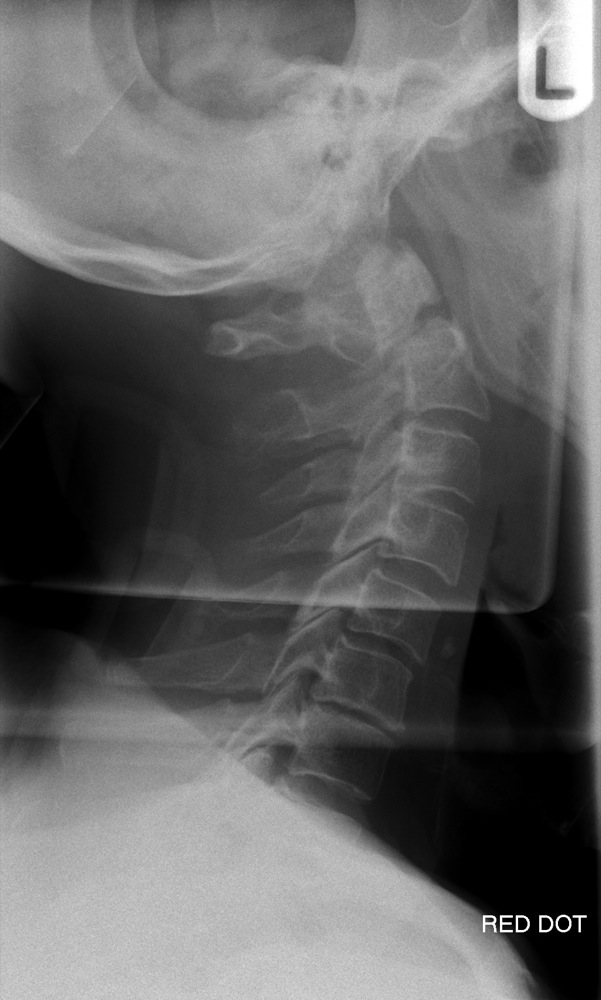
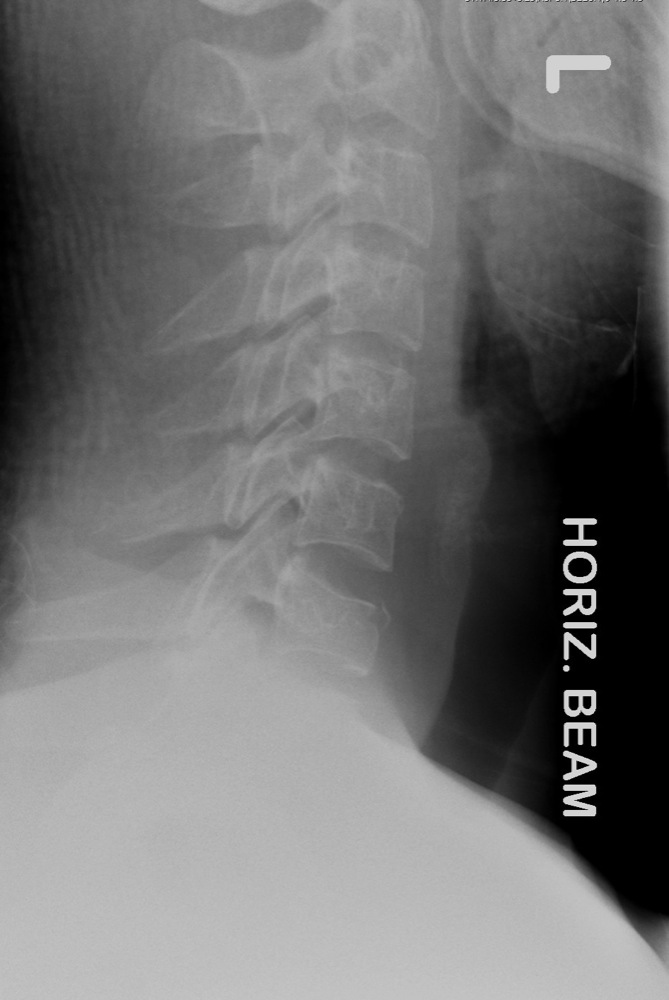
Sudden deceleration of the body, with flexion and extension movements of the cervical spine usually results in sprain or intervertebral disc injury without fracture or dislocation. The commonest radiographic appearance is straightening of the cervical spine due to severe muscle spasm, with the normal curvature reduced or reversed:

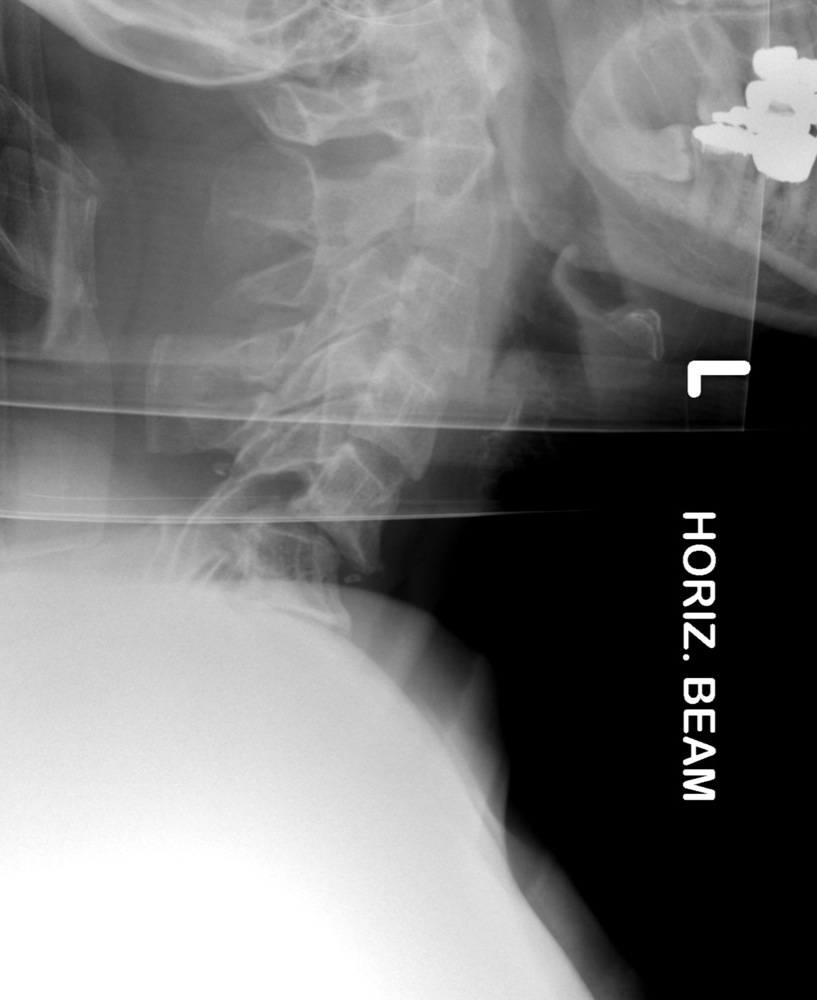
Refers to soft tissue injury. Anterior subluxation occurs with disruption of the posterior longitudinal ligament, the interspinous ligament and the intervertebral disc. The lateral projection demonstrates localised kyphotic angulation with an increase in height of the intervertebral disc posteriorly and associated fanning of the spinous processes.
The converse of hyperflexion strain; the anterior longitudinal ligament is disrupted as evidenced by widening of the intervertebral disc space anteriorly. The facet joints are disrupted and the interspinous distance is narrowed.
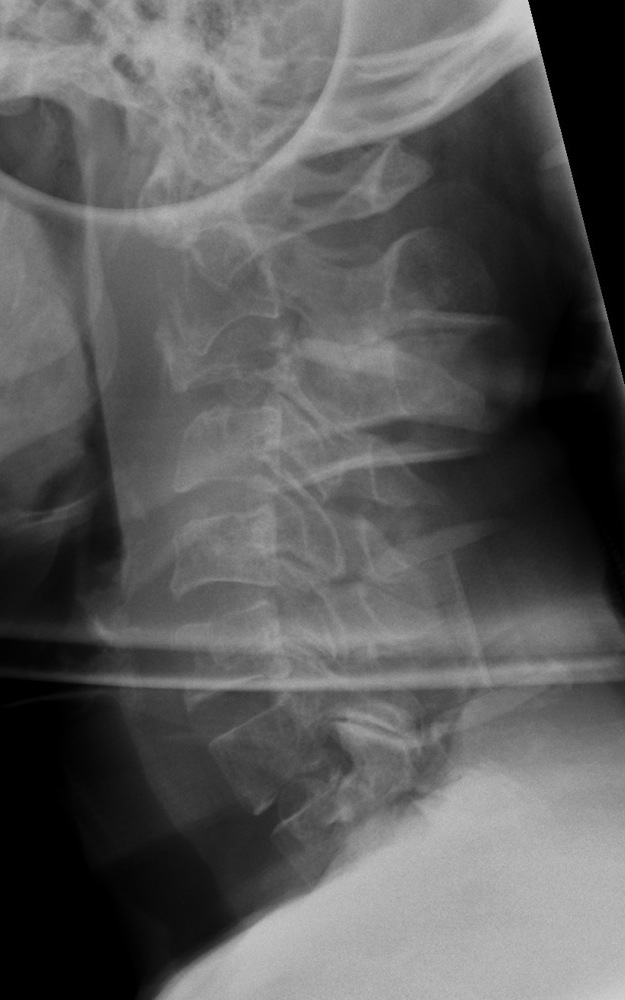
Refers to degenerative changes of the intervertebral disc spaces, which is demonstrated by disc space narrowing, endplate sclerosis and osteophyte formation. Facet joint OA is seen posteriorly. The associated osteophytes may impinge on the nerve root foramina. The appearance of striking degenerative changes within the cervical spine may obscure underlying injury. It is therefore important to search for co-existant trauma. A common mechanism of injury in those patients with spondylosis (often the elderly) is a fall directly onto the forehead with a subsequent fracture at C2:



Primary tumours can metastasise to the vertebral bodies demonstrating a lucent, moth-eaten, permeative appearance. There is often subsequent collapse:

It is not unusual to see a congenital fusion within the cervical spine, usually at C2/C3 with fusion of the vertebral bodies and posterior elements. This is often associated with a hypoplastic odontoid peg: