Heidi Nunn (Advanced Practice Reporting Radiographer)
Higher data usage mode: Magnified images are currently set to load all at once - this will give the best viewing experience, but may use more data. You can change this setting in the "Modules" menu, or here.
Assess skeletal radiographs using a systematic approach
Use common lines which are helpful in interpreting the image
Understand importance of good radiographic positioning
Describe tarsal, metatarsal and phalangeal anatomy
Understand mechanisms of injury and the likely fractures/dislocations which may result
Search for subtle injuries and understand their clinical significance
Accurately describe dislocations and associated fractures
Understand common eponyms
Understand paediatric anatomy
Recognise normal variants and their significance (eg, accessory ossicles)
Normal anatomy
DP radiograph - The medial border of the base of the 2nd metatarsal should be in line with the medial border of the middle cuneiform. There is overlap of the lateral metatarsal bases and tarsal bones (cuboid and lateral cuneiform).
Oblique radiograph - The medial border of the base of the 3rd metatarsal should be in line with the medial border of the lateral cuneiform. Now the 1st/2nd mt bases, and the medial and middle cuneiforms overlap:
Os calcaneus secundarius - adjacent to the anterior process of the calcaneum:
Os intermetatarseum - between 1st and 2nd metatarsals:
Hallux sesamoids - these are often bipartite:
Phalanges
Fractures and dislocations are common. Magnification and correct windowing of the image is often necessary for detection.
Fifth metatarsal fractures
Avulsion fractures are common at the tuberosity at the base of the 5th metatarsal. This is at the insertion of the peroneus brevis tendon, and avulsions occur due to inversion injuries:
Jones fracture - refers to a transverse fracture of the proximal shaft of the 5th metatarsal. Has a poorer prognosis and different treatment to avulsion fractures (requires non-weight bearing).
Beware in children the normal unfused apophysis. This should not be mistaken for a fracture, by observing that the apophysis lies longitudinal to the long axis of the metatarsal. A fracture line will run transversely:
The normal apophysis may appear displaced and/or fragmented. However this is usually normal:
An apophysis is located at a site of ligament or tendon attachment. The apophysis does not contribute to the longitudinal growth of bone. This differs from an epiphysis which is located adjacent to a joint and does contribute to longitudinal growth.
Stress fractures of the metatarsals
Radiographic findings are often not evident initially, however approx. 10 days later a transverse radiolucency indicates the site of fracture followed by periosteal reaction and fluffy callus formation indicating healing. Profuse callus formation often subsequently develops. Usually 2nd/3rd distal metatarsal shaft affected:
Injuries of the tarsal bones
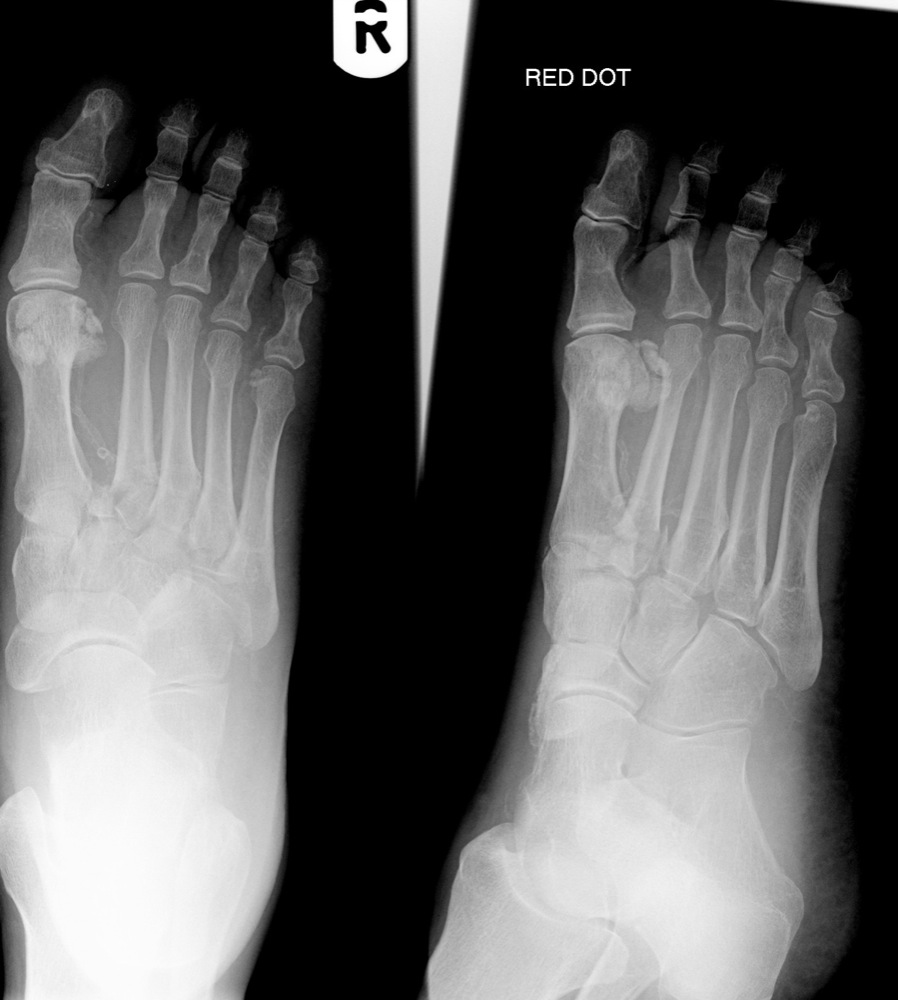
Check the lateral cortex of the cuboid for subtle avulsion fractures:
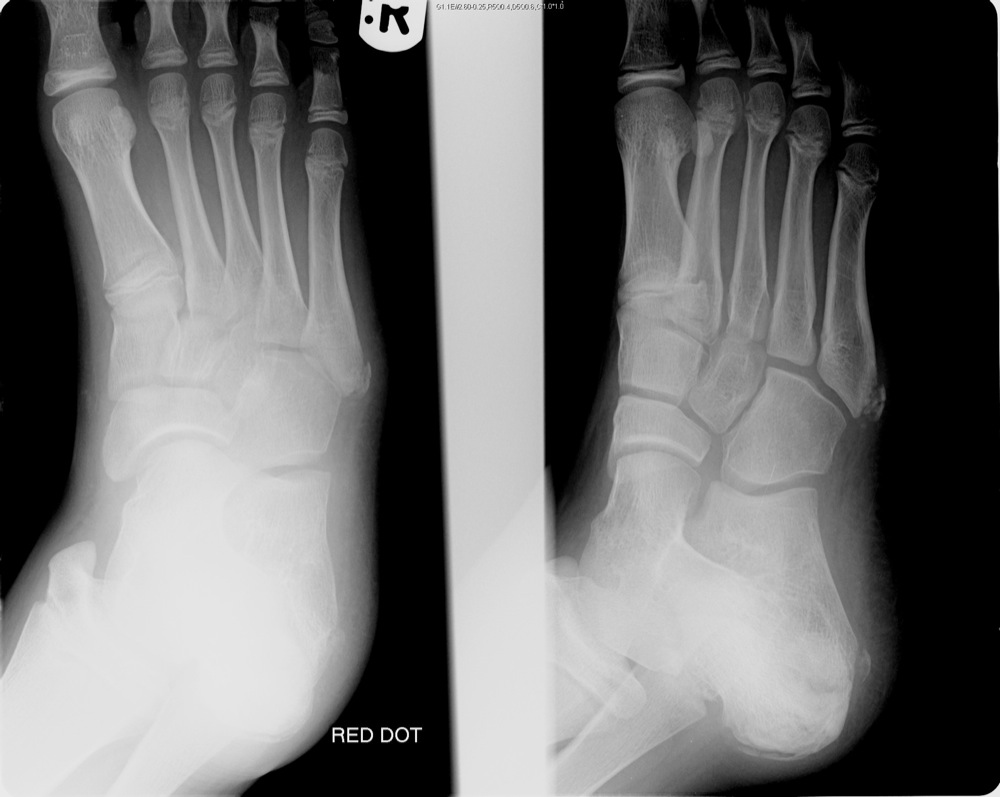
Avulsion fractures of the dorsal surface of the navicular and head of talus are common and often missed. These can only be identified by a lateral view:
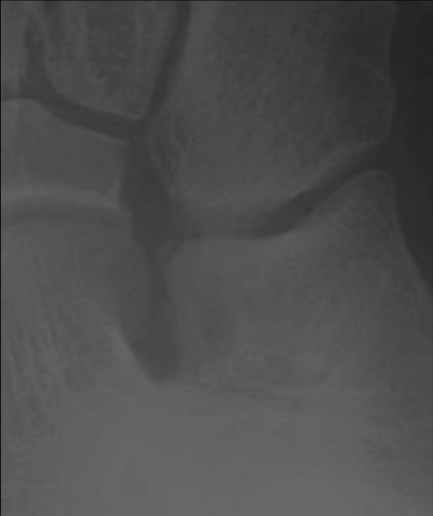
Avulsion of the anterior process of the calcaneum by the bifurcate ligament is relatively common but can be subtle, resulting from an inversion injury. This is usually seen on the oblique view of the foot:
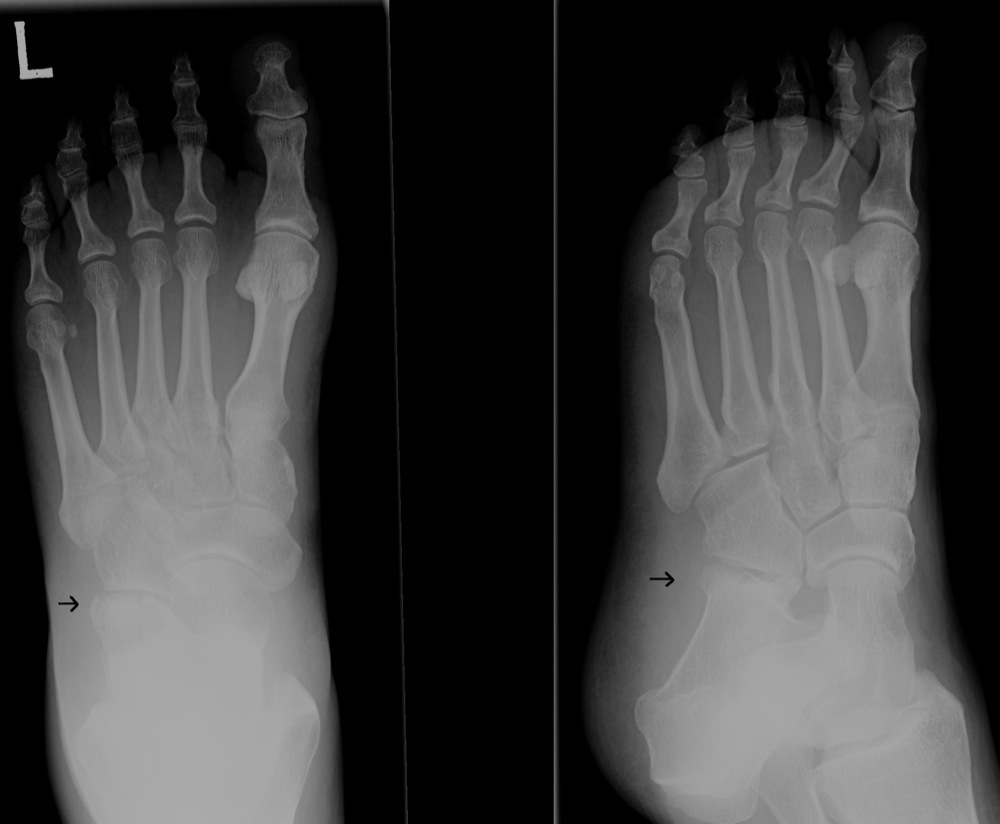
A second common avulsion site of the calcaneum is seen laterally (on the DP foot) at the insertion of the extensor digitorum brevis muscle:
Injuries to the anterolateral aspect of the calcaneum may be very subtle but, if missed, can be debilitating:
Lisfranc fracture-dislocation (tarso-metatarsal)
Refers to fractures at the base of the metatarsals (usually the 2nd) accompanied by lateral subluxation at the tarso-metatarsal joints. The base of the 2nd metatarsal is held in a mortise by the three cuneiform bones. When it is fractured distal to this, the base often remains held in the mortise by the ligaments, with lateral subluxation of the metatarsals:
This injury may be subtle. However, by observing the alignment at the base of the 2nd and 3rd metatarsals with the adjacent cuneiforms, this significant injury should not be missed.
Midtarsal (Chopart) fracture-dislocation
Disruption of the talonavicular and calcaneocuboid joints, with medial or lateral dislocation of the foot. Occurs due to high velocity trauma; these injuries are usually easy to detect as the foot is obviously deformed: