




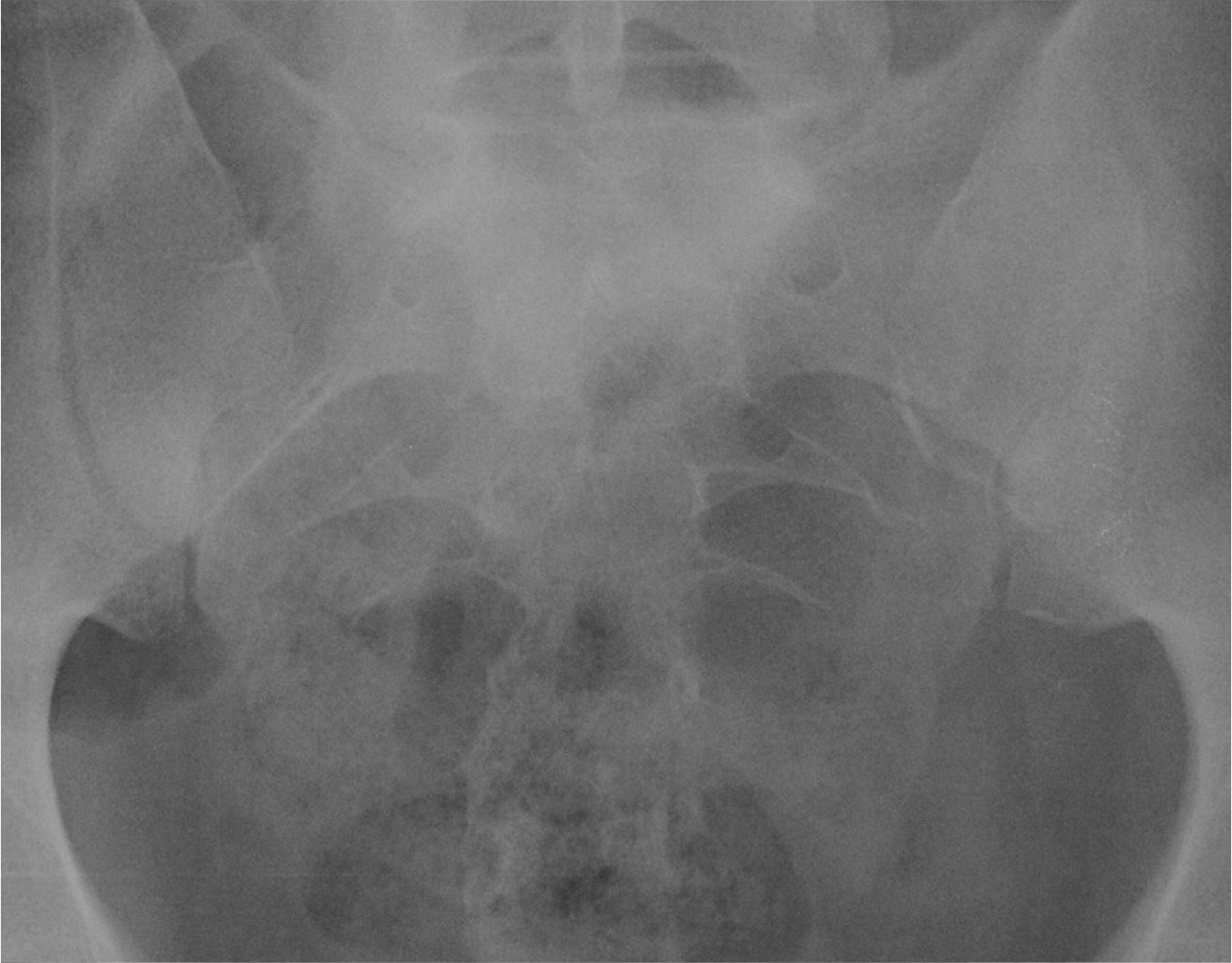


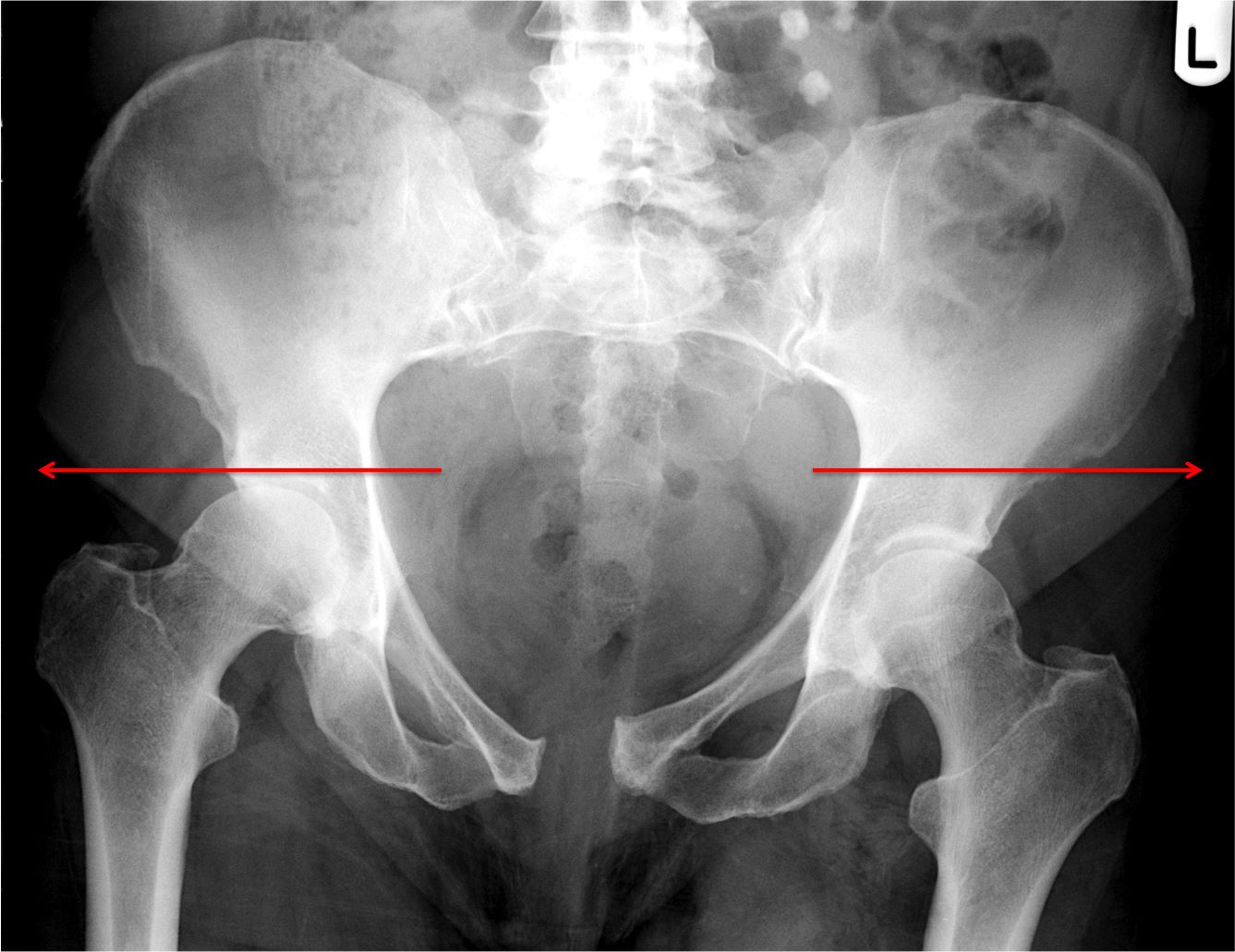
An anterior compression force results in disruption of the SI joints (>4mm), diastasis of the symphysis pubis (>5mm) and external rotation of the hemipelvis. Also known as an "open book" injury:



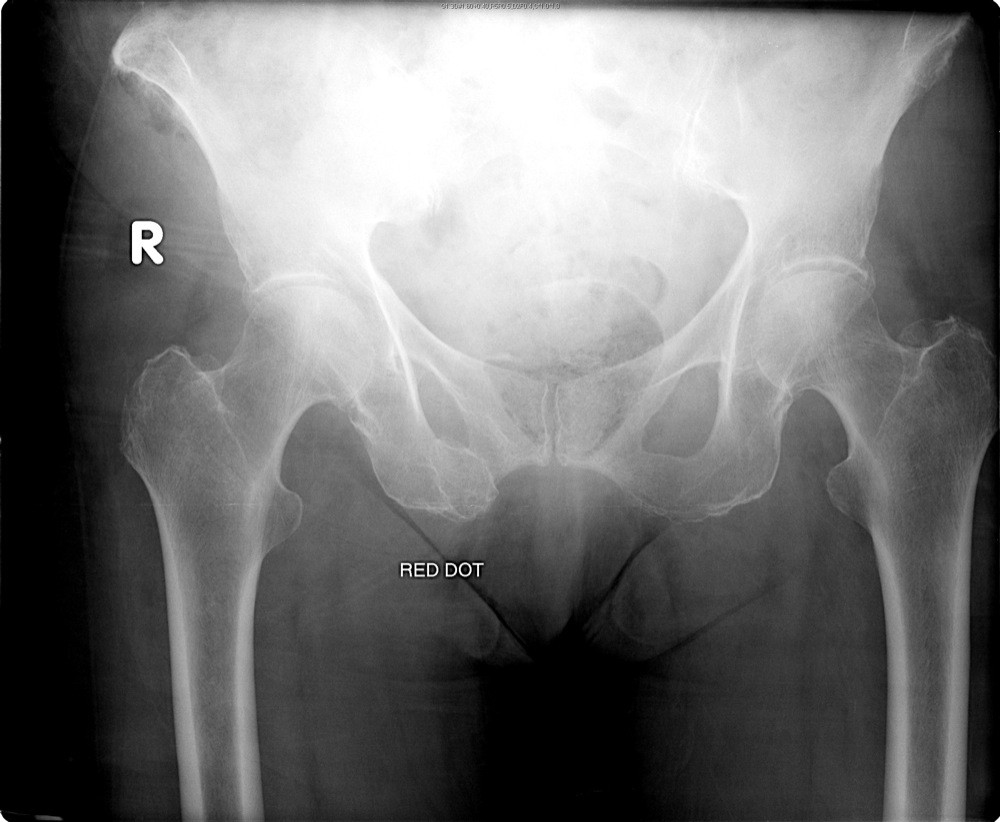
A lateral compression force results in oblique fractures of the pubic rami bilaterally (with overlapping fragments), impacted fractures of the sacral foramina ipsilateral to the force, with infolding of the hemipelvis:


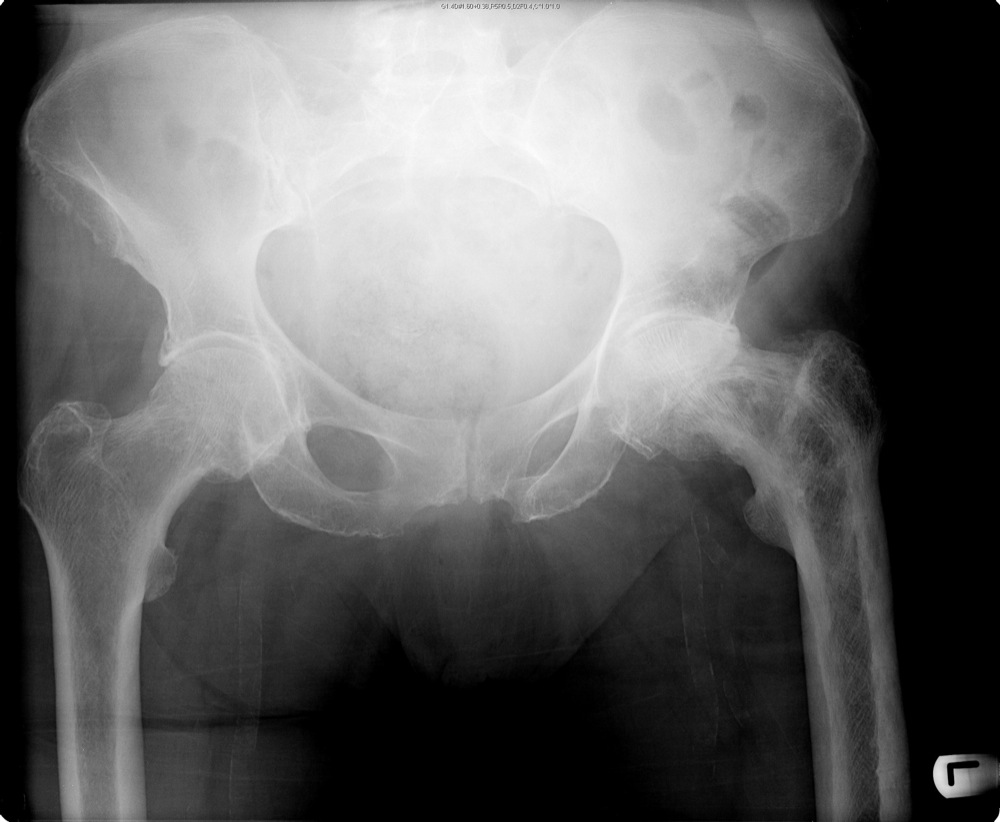
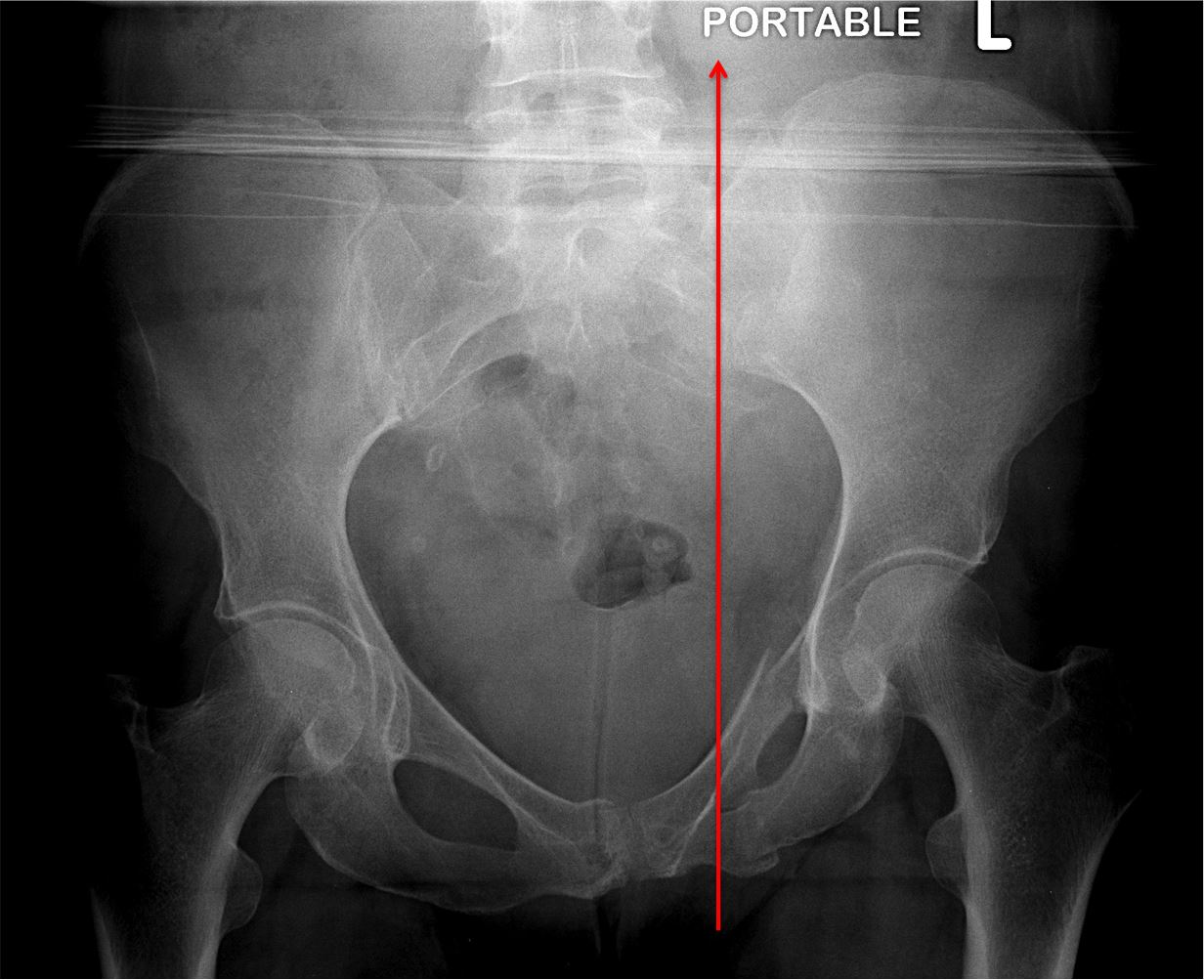
A vertical shearing injury results in vertical, unilateral fractures of the pubic rami, vertical fracture of the sacral foramina on the same side (or fractured ileum paralleling SI joint/disruption of the SI joint) with the hemipelvis usually displaced superiorly:

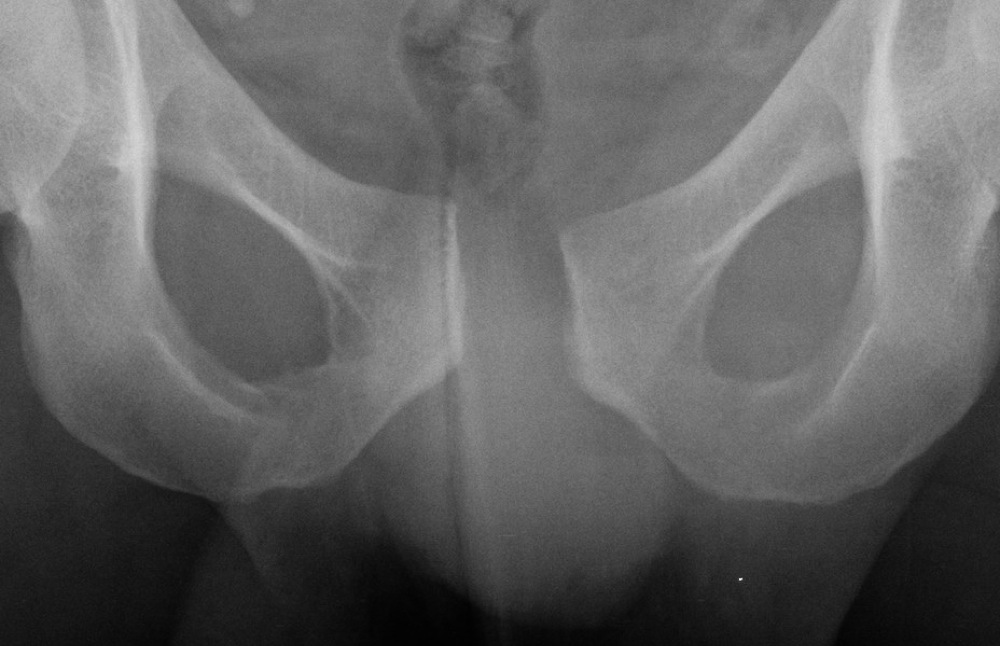
A straddle injury refers to a force against the perineum. This results in fractures of all pubic rami bilaterally with the central fragment displaced superiorly.







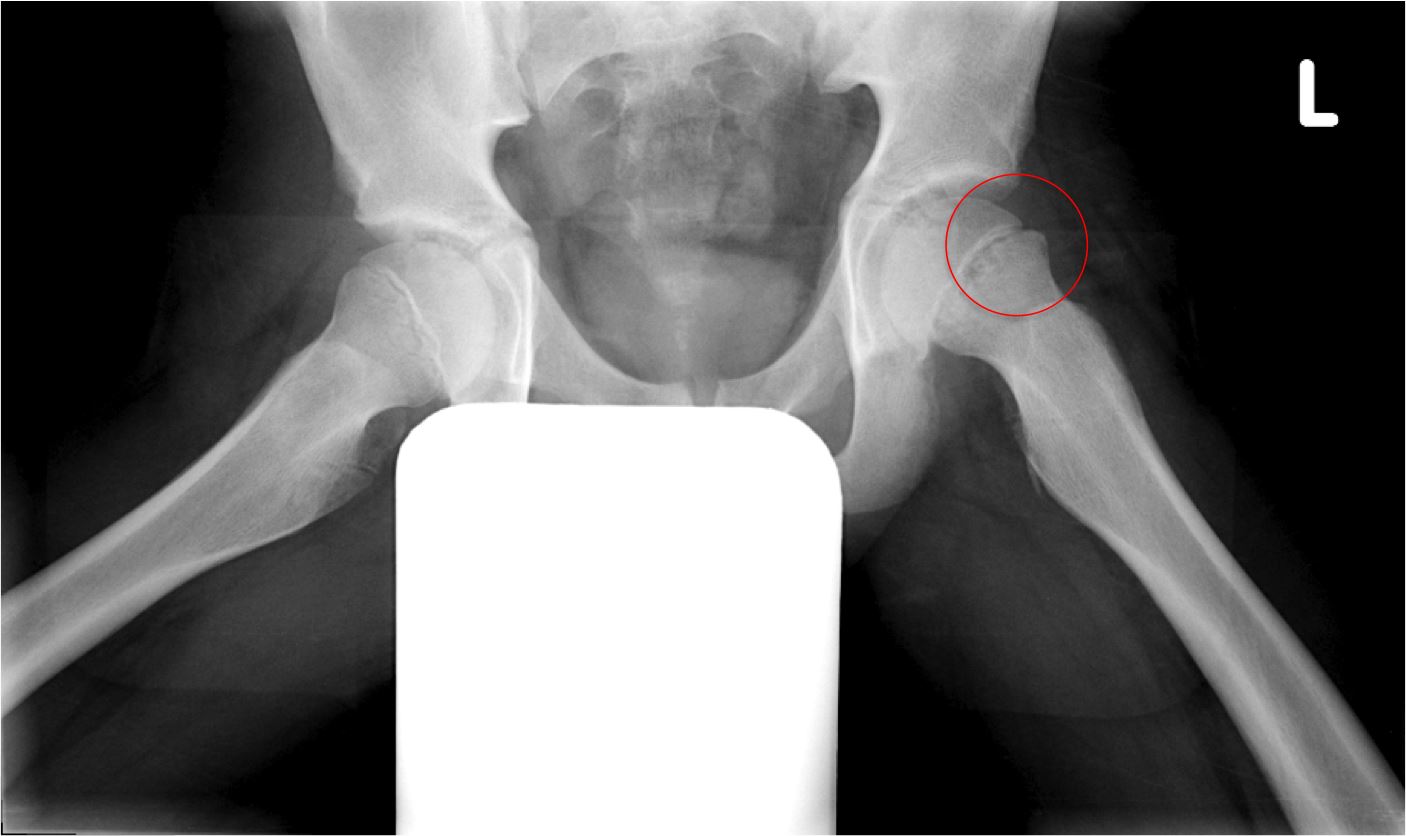
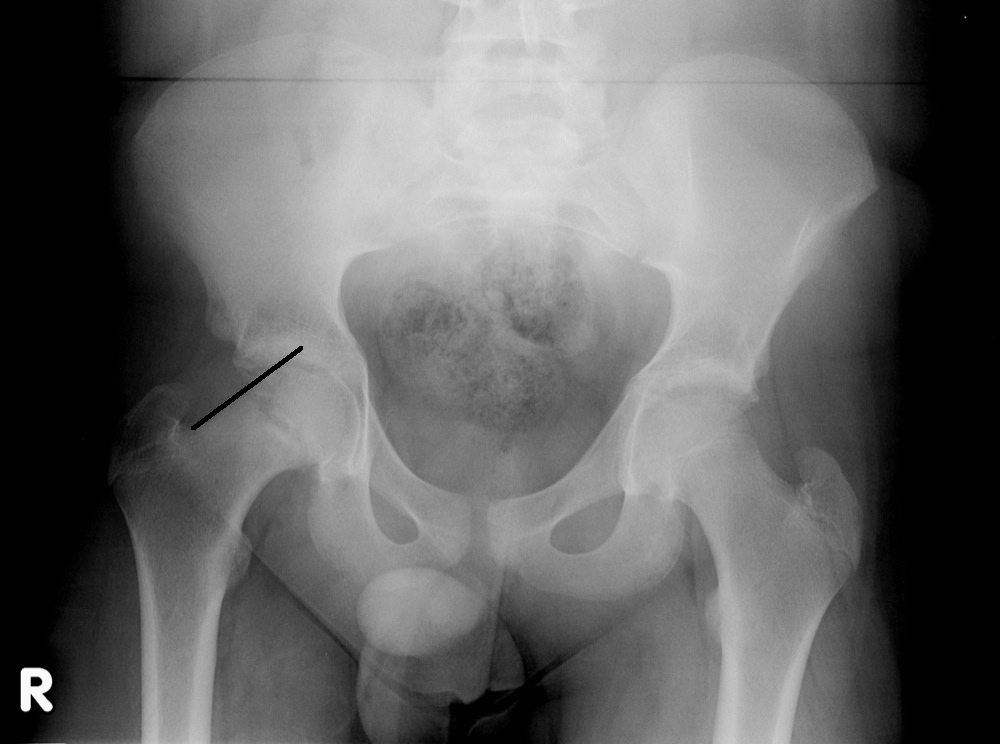
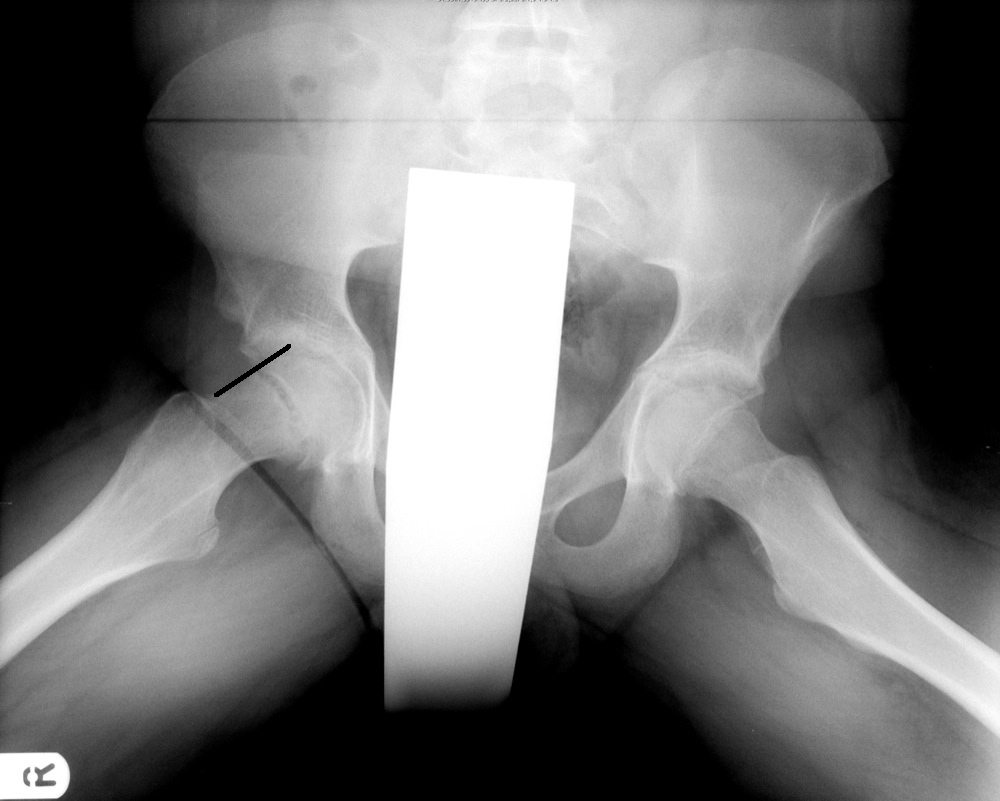
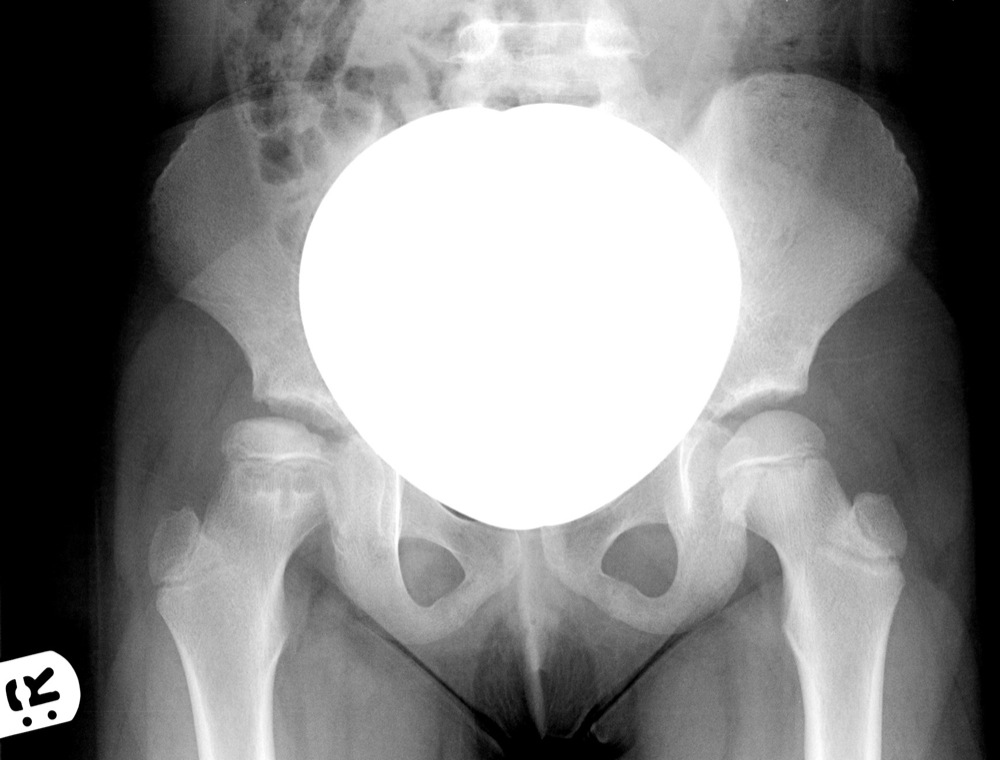
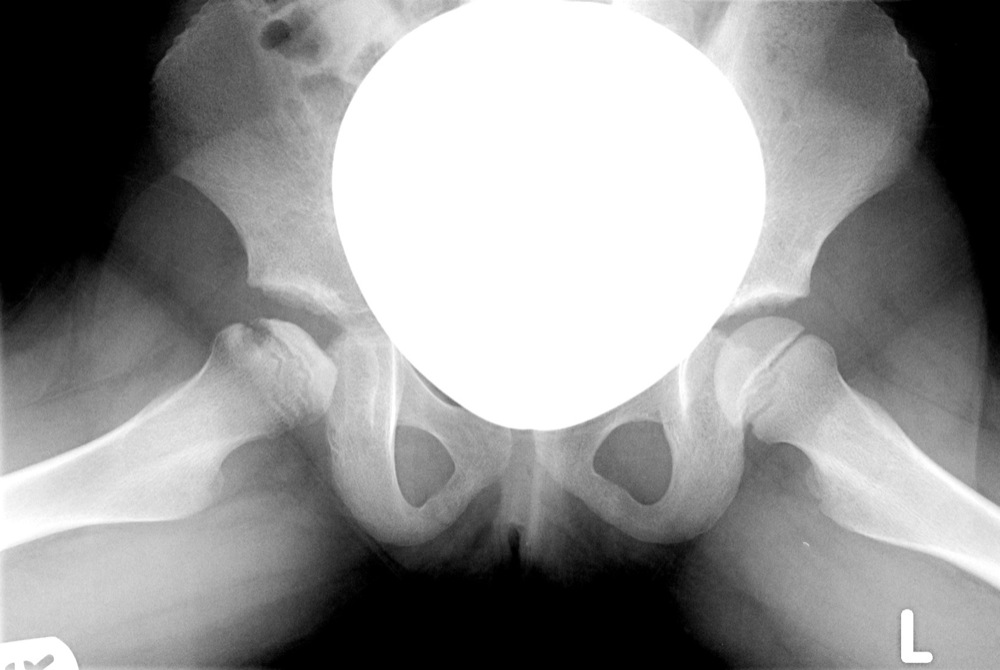
| Perthes' | Femoral Head |
| Osgood Schlatter's | Tibial tuberosity |
| Kienböck's Malacia | Lunate |
| Freiberg's | Metatarsal head |
| Sinding Larsen | Patella |
| Scheuermann's | Vertebral epiphysis (apophyseal rings) |
| Calve's | Vertebral body |
| Köhler's | Navicular |
| Sever's | Calcaneum |





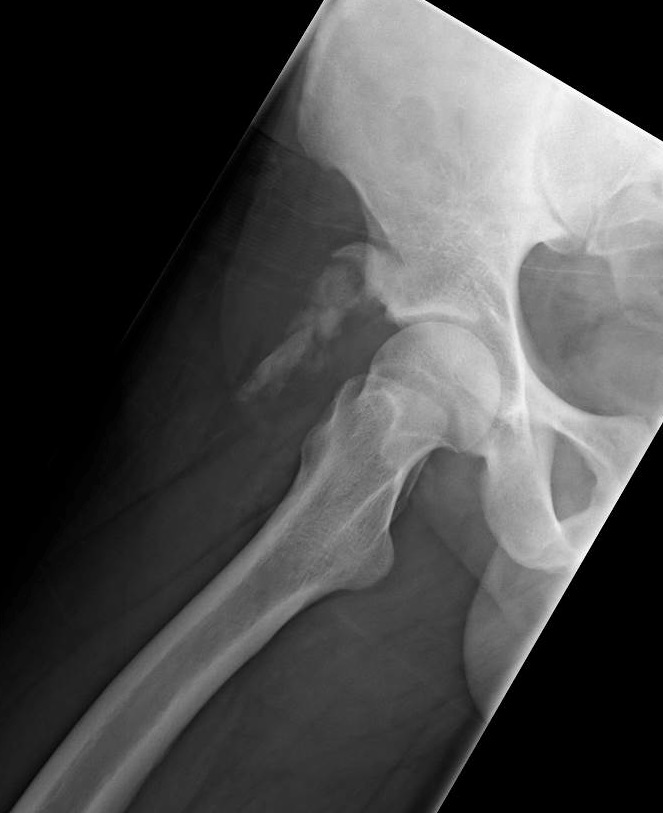
Bone is expanded.
The cortex is thickened.
The trabeculae is coarse.