Compression fracture at thoracolumbar junction + fractures of the os calcis.
Upper thoracic spine wedge fractures + sternum fractures.
Assess on both images:
- Height of vertebral bodies should be equal.
- Width of intervertebral disc spaces should be uniform.
- Continuity of superior and inferior endplates: should remain unbroken.
- Distance between spinous process should be equal.
- Trace the posterior elements; the pedicles, laminae, and spinous processes.




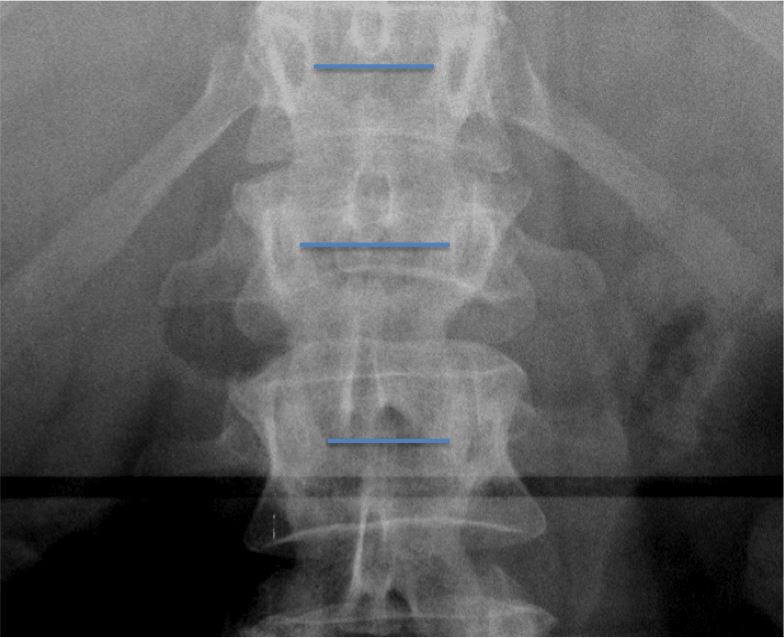
Specifically on the AP image:
- Soft tissue signs - Widening of the paraspinal line adjacent to the left side of the thoracic spine is indicative of a haematoma resulting from a fracture:
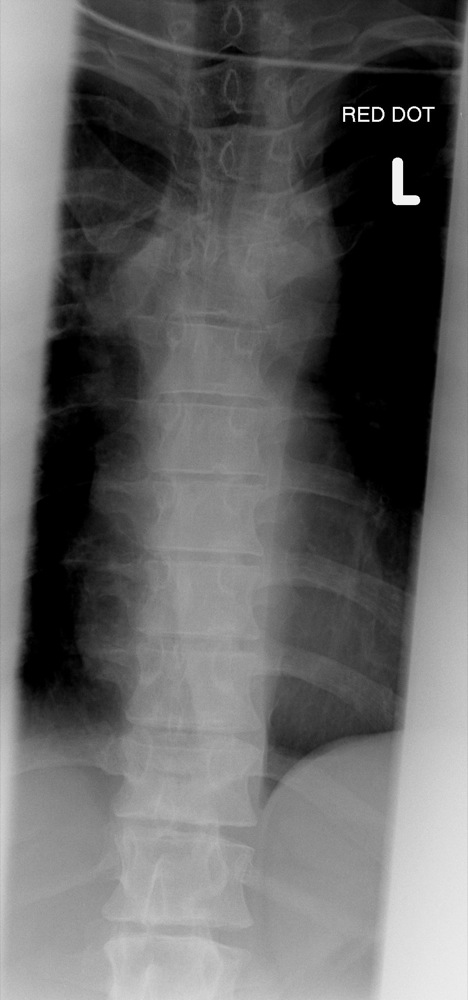
- Pleural cap - Refers to a paraspinous haematoma, which dissects over lung apex.
- Inter-pedicular distance. Should become gradually wider from L1 to L5.
- Check for an "empty" vertebral body on the AP radiograph; the posterior elements should be superimposed.
- Transverse processes should remain intact.
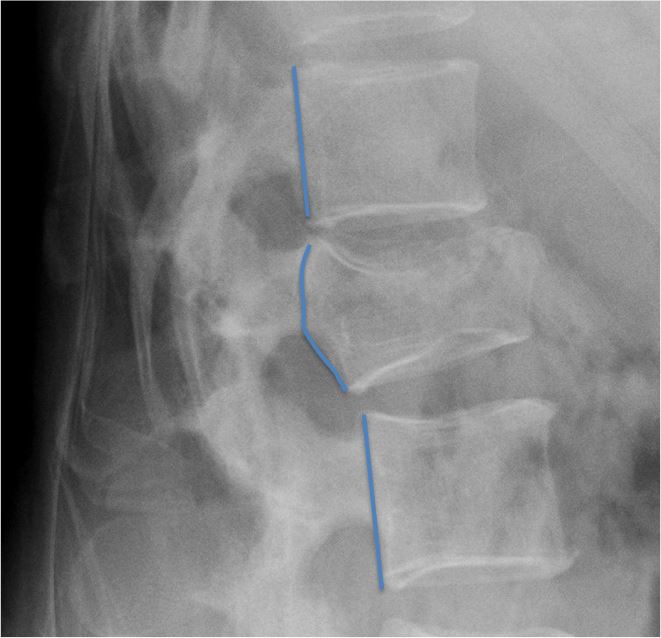
Specifically on the lateral image:
- Malalignment. Trace the anterior, posterior and spinolaminar lines. If two of these lines are disrupted, the injury is considered unstable.
- Posterior vertebral body cortex should be slightly concave.
Forward flexion causes wedge compression deformity of the anterior vertebral body, with the normal posterior concavity of the vertebral body remaining intact. Often occurs in association with fracture to the superior endplate:


Initially may appear to be an anterior wedge compression fracture, however closer inspection of the lateral view will demonstrate retropulsion of a fragment of the posterior vertebral body into the spinal canal. This may be subtle and a loss of the normal concavity of the posterior vertebral cortex may be the only indication. AP may demonstrate widening of the inter-pedicle distance, often with a sagittal fracture of the inferior half of the vertebral body. High probability of neurological deficit.
May occur with use of lap belt during a deceleration injury. Refers to compression fracture of the vertebral body with transverse/horizontal fractures of the posterior elements:


With an increase in distraction, the AP will demonstrate an "empty" vertebral body, as the posterior elements will not be superimposed on the vertebral body. There will be an increase in the inter-spinous distance and a break in continuity of the pedicles or spinous process. Lateral will show an increase in the inter-spinous distance with horizontal fractures of the spinous process/lamina/pedicles running into the vertebral endplates.
The anterior and posterior vertebral lines will demonstrate malalignment, with disruption of the facets posteriorly. Occurs in association with anterior wedging of the vertebral body below, with a characteristic triangular fragment arising from the antero-superior margin. Lateral dislocations are also seen. High probability of neurological deficit:


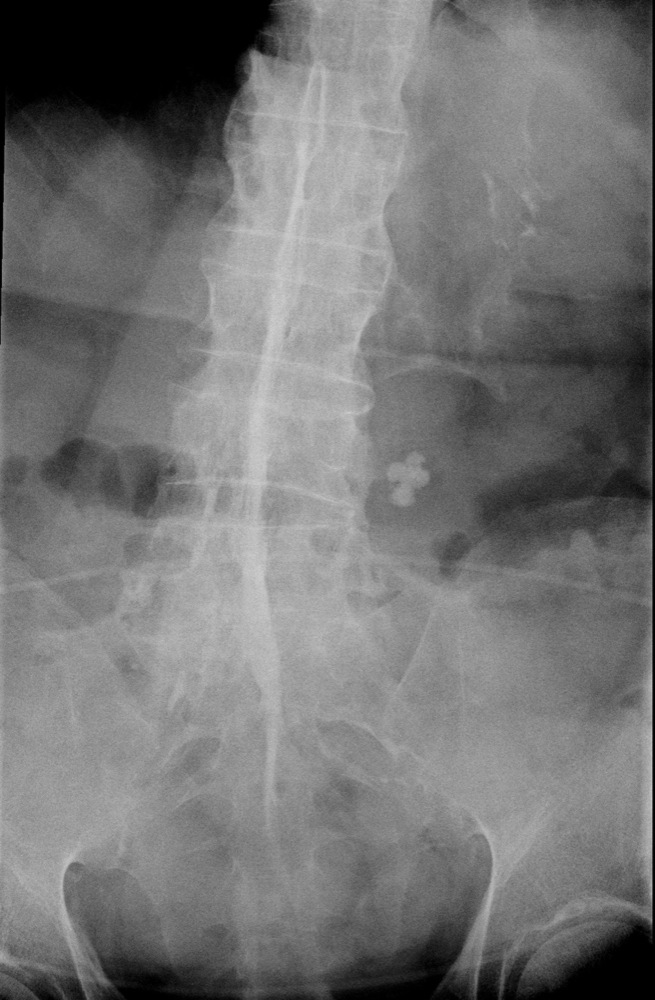
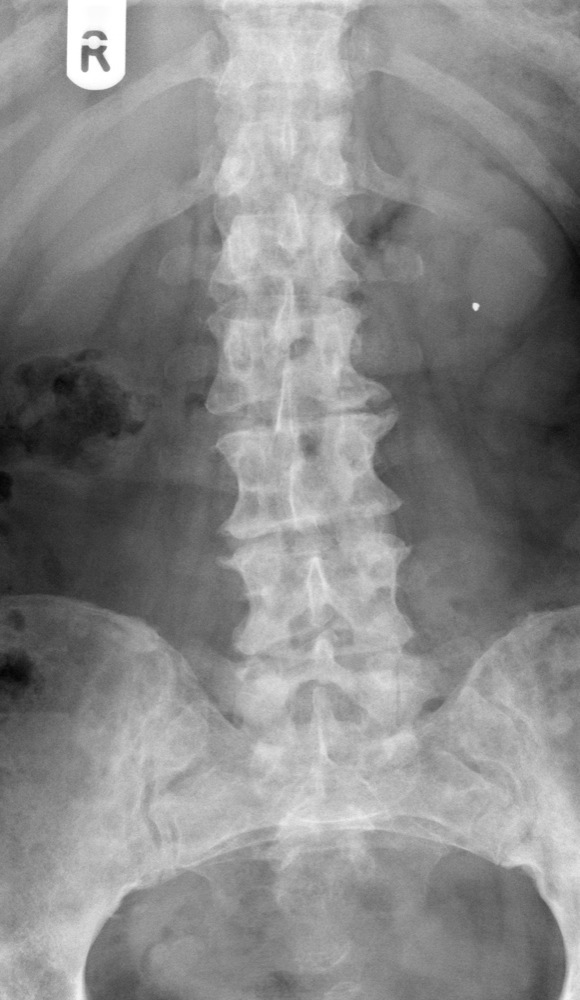
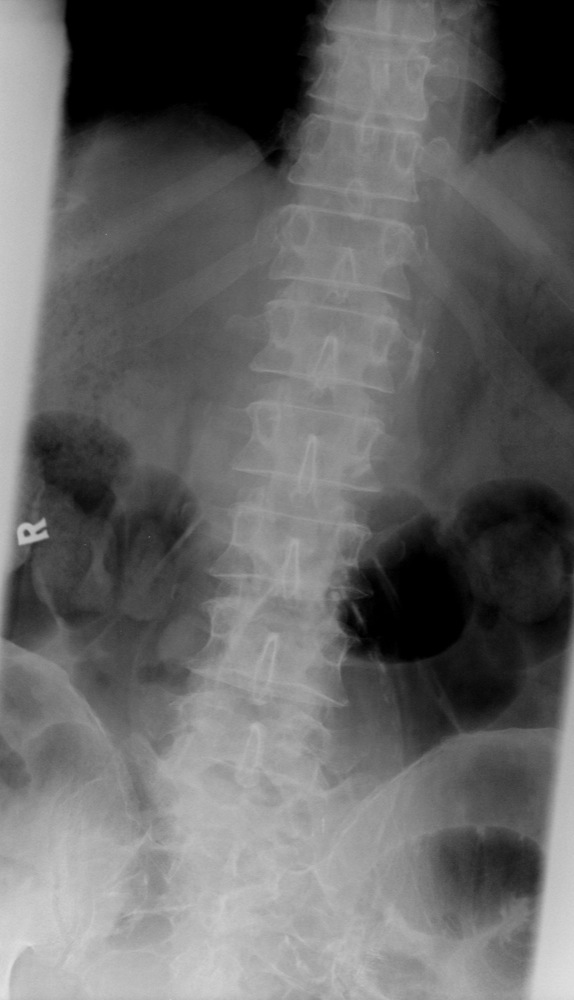
Fractures may occur to transverse processes. These are often subtle and may only be seen through careful windowing of the image. Overlying bowel gas often obscures image detail:

Refers to degenerative changes of the intervertebral disc spaces, which is demonstrated by disc space narrowing, endplate sclerosis and osteophyte formation. Facet joint OA is seen posteriorly. The associated osteophytes may impinge on the nerve root foramina.




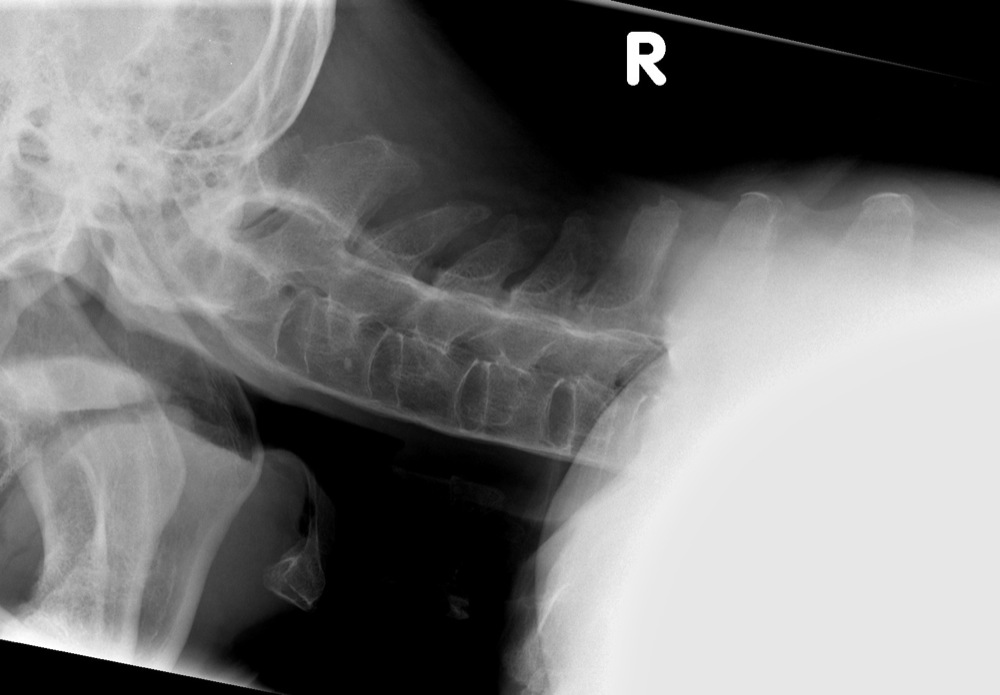
A fracture that may be acute or chronic in origin, that extends from the inferior facet across the pars interarticularis, to the superior facet (the pars interarticularis is the area of the lamina that lies within the facets). This defect may be bilateral and may lead to a spondylolisthesis. Spondylolysis is evident on an oblique radiograph by identifying the "Scotty dog":
|
Nose
|
= | Transverse process |
|
Eye
|
= | Pedicle |
|
Ear
|
= | Superior facet |
|
Front leg
|
= | Inferior facet |
|
Collar through neck
|
= | Fracture |



A forward displacement of one vertebra upon another. May be due to:
Trauma
Congenital weakness of the pars interarticularis
Degenerative facet joint diseaseMay not be symptomatic, however, if severe, may cause foraminal stenosis, causing nerve root impingement. Consequently it will be treated surgically. Grade I refers to a displacement of up to 25%, and a grade II refers to malalignment of 25-50%:

The lumbar spine is often affected. There are three key features:
Bone is expanded
The cortex is thickened
The trabeculae is coarse

Primary tumours may metastasize to the vertebral bodies. May either demonstrate a "moth-eaten", permeative appearance:

or, specifically to the lumbar spine, an "ivory vertebra":


or destruction of the pedicle:


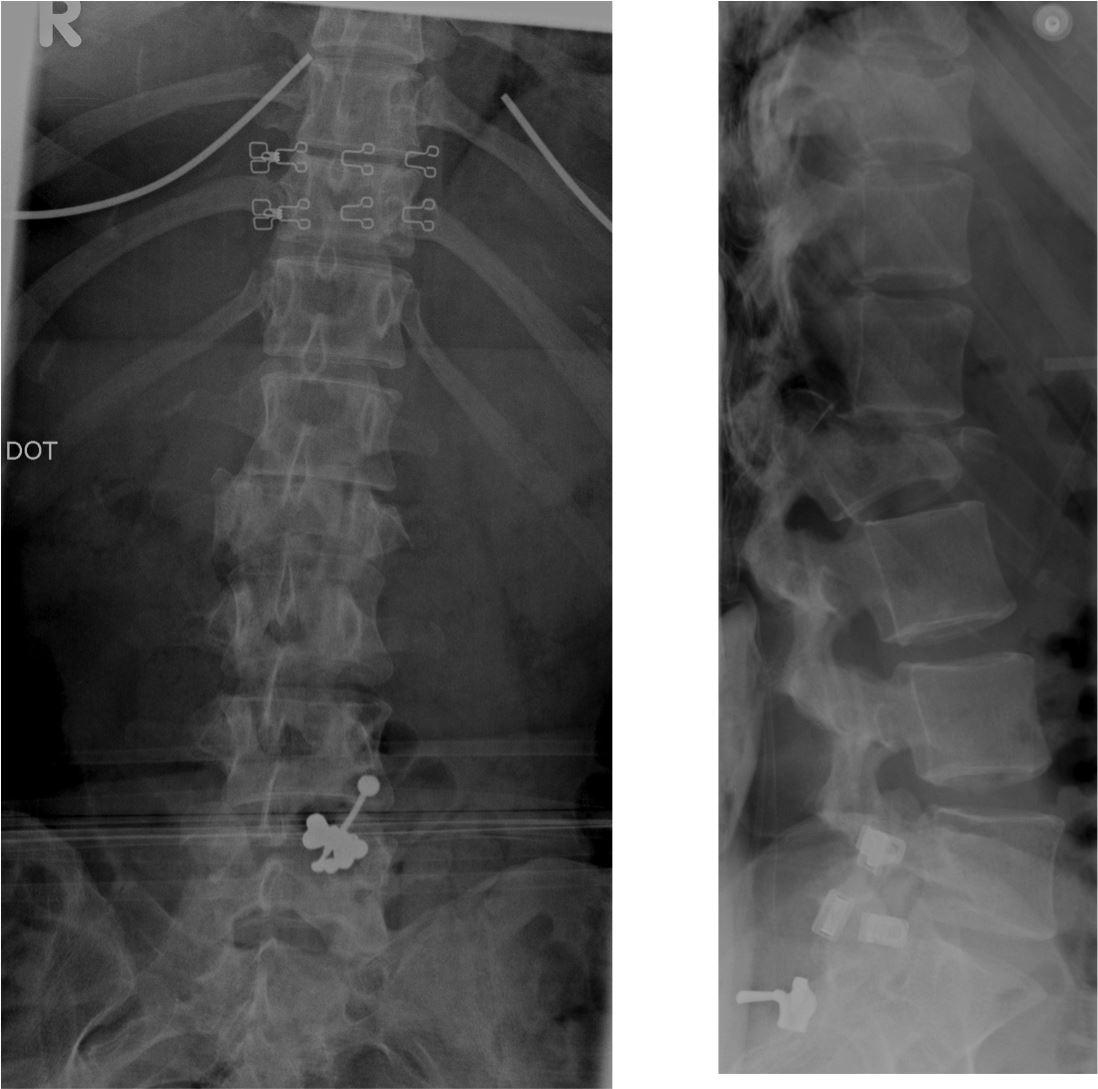
Attendance to casualty with back pain may be due to an abdominal aortic aneurysm. This may be demonstrated on either AP or lateral lumbar spine radiographs, if the aorta is calcified:

Refers to calcification of the anterior and posterior longitudinal ligaments and intervertebral discs resulting in fusion of the spine from the sacroiliac joints up through the thoracolumbar spine to the cervical spine. This "bamboo spine" may fracture: