When interpreting whether an image is normal or abnormal, it is common to come across incidental lytic lesions, which, depending on their appearance, must be classified as either a normal variant, or something which warrants further investigation.
It is difficult to determine radiologically with plain radiograph imaging if a lytic lesion is benign or malignant. It is more accurate to describe whether the process looks aggressive or non-aggressive. Some factors, as outlined below, help to determine whether a lesion looks aggressive or non-aggressive, and therefore the differential diagnosis.
It is important to remember, however, that some benign processes such as osteomyelitis, can mimic malignant tumours, and some malignant lesions, such as metastases or myeloma, can look benign.
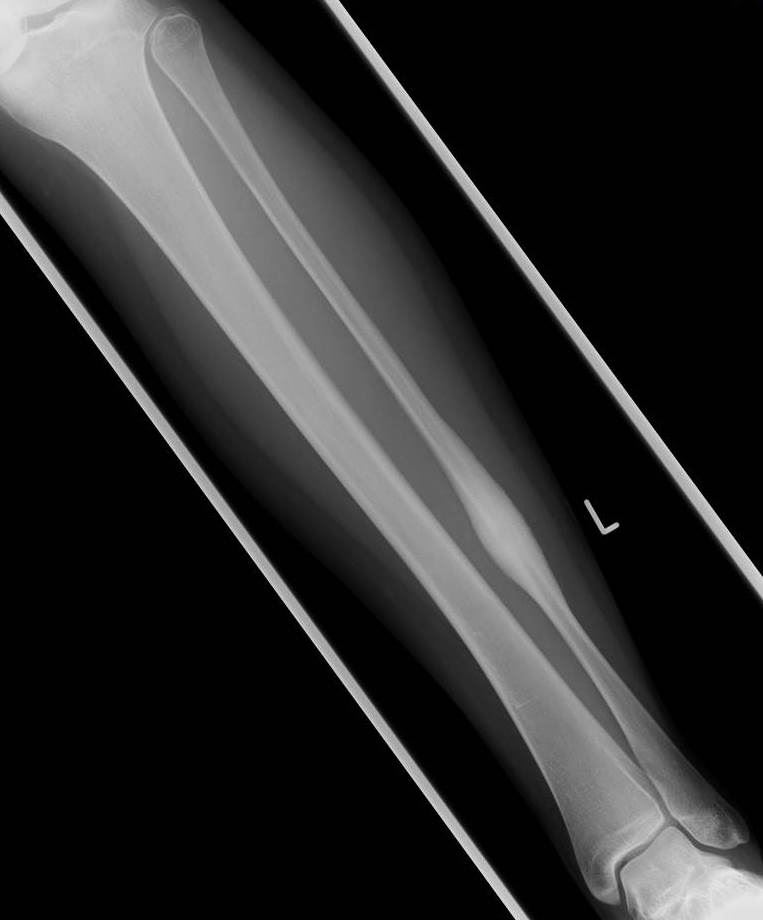
- Benign periostitis looks thick, wavy, dense and uniform, as it is slow growing and therefore gives the periosteum time to lay down new bone
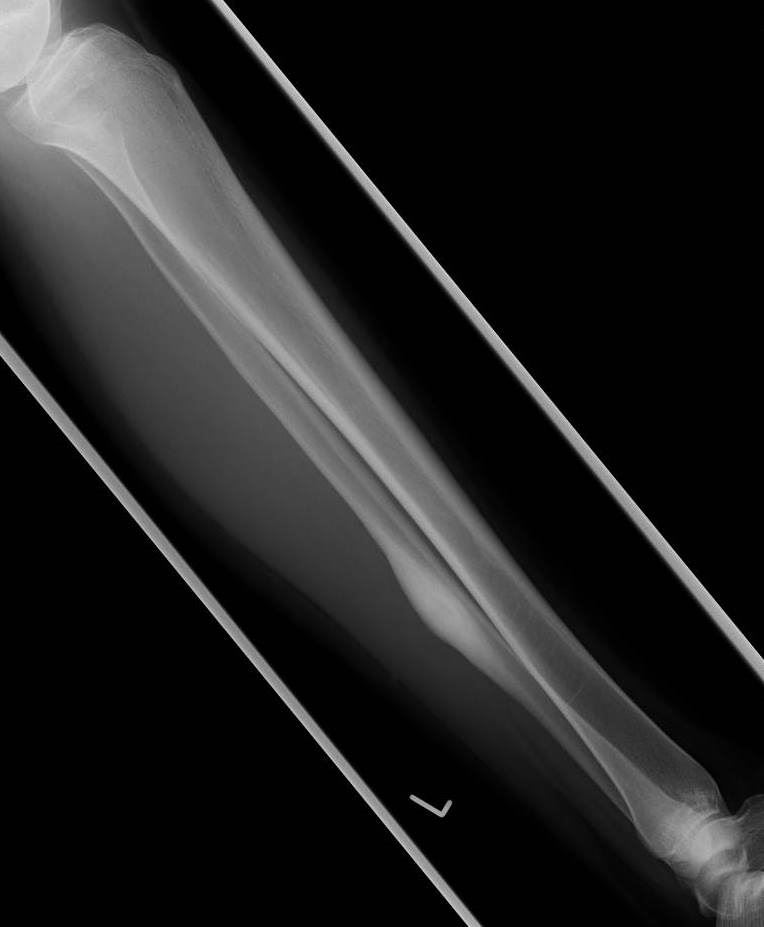
- Aggressive periostitis is often described as lamellated (onion-skinned), amorphous and sunburst as the periosteum does not have time to consolidate