



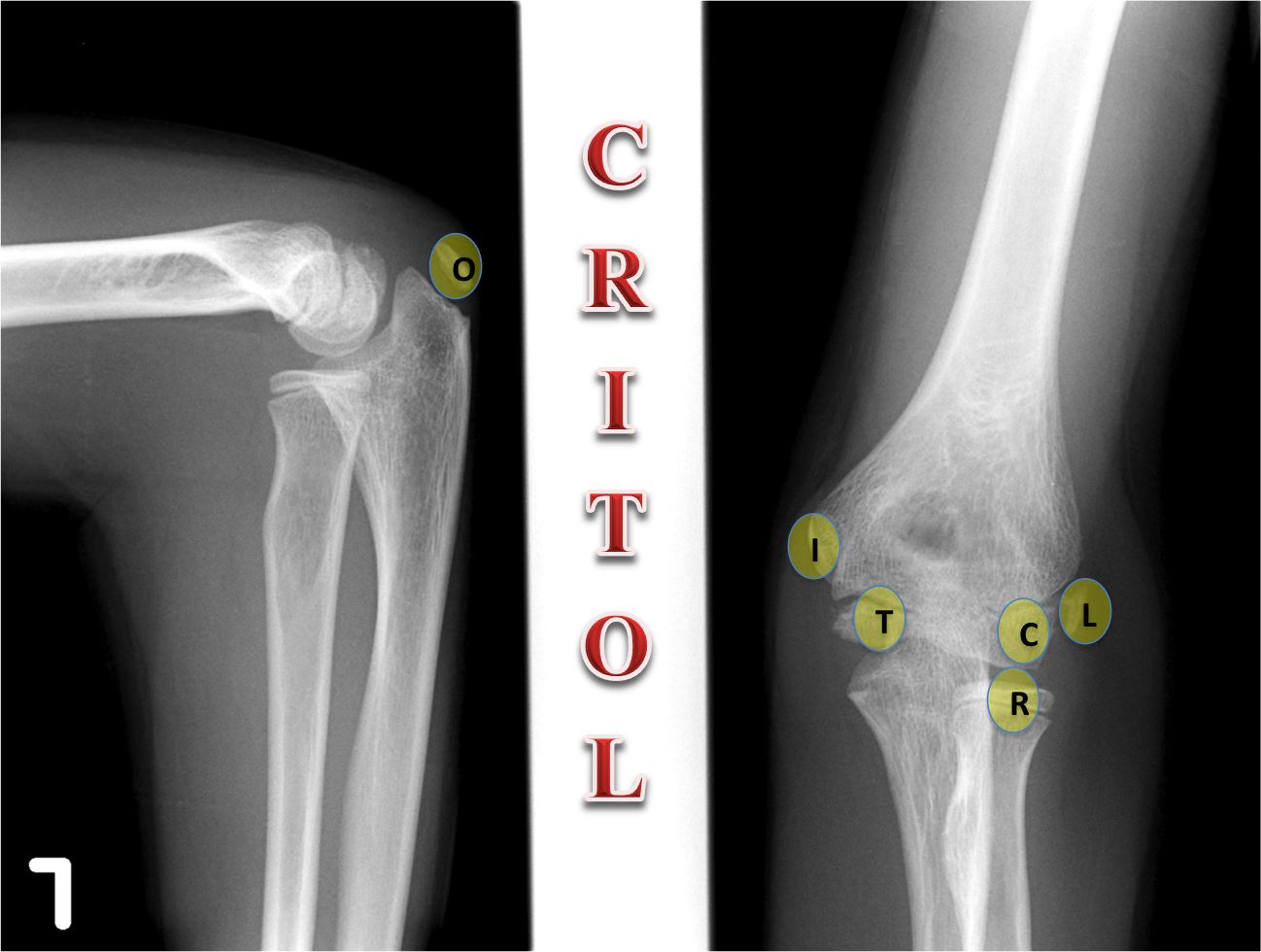
| C = CAPITELLUM R = RADIAL HEAD I = INTERNAL EPICONDYLE (MEDIAL) T = TROCHLEA O = OLECRANON L = LATERAL EPICONDYLE |
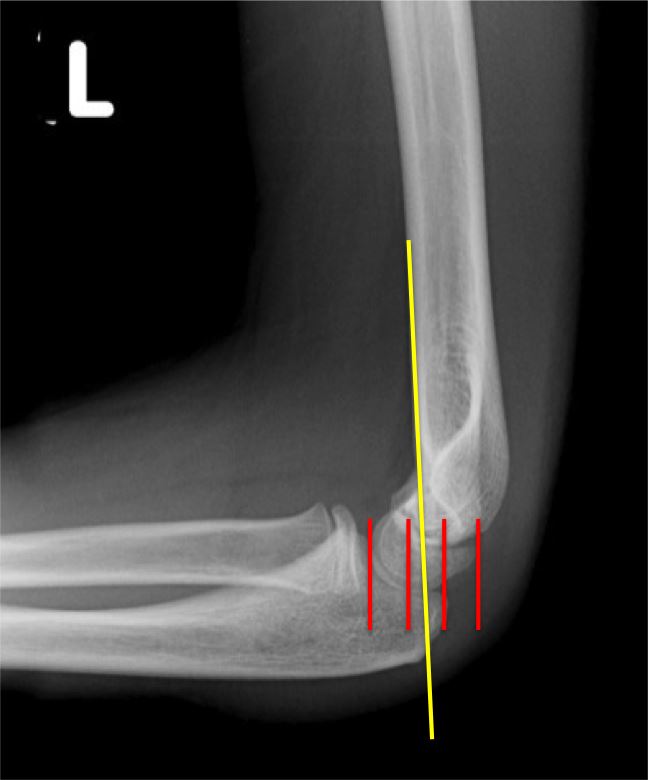
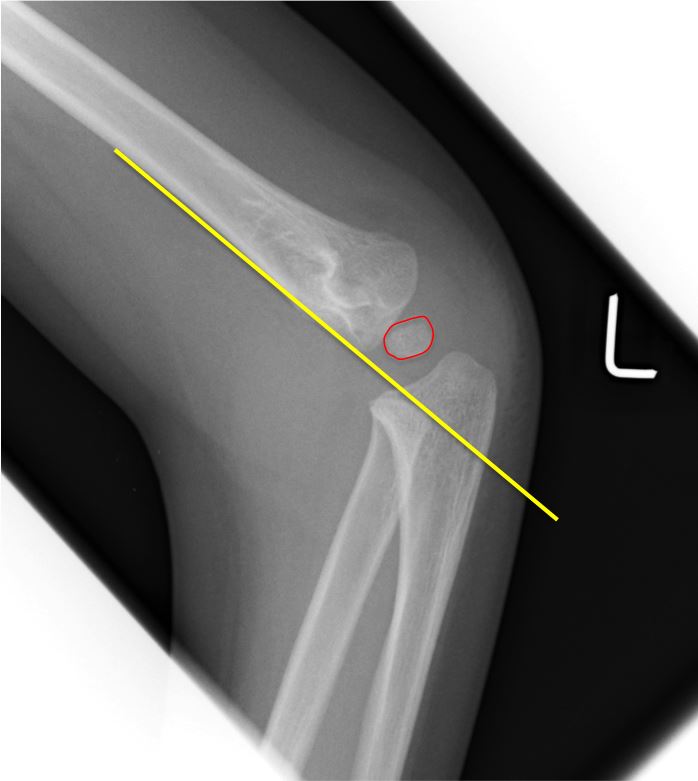
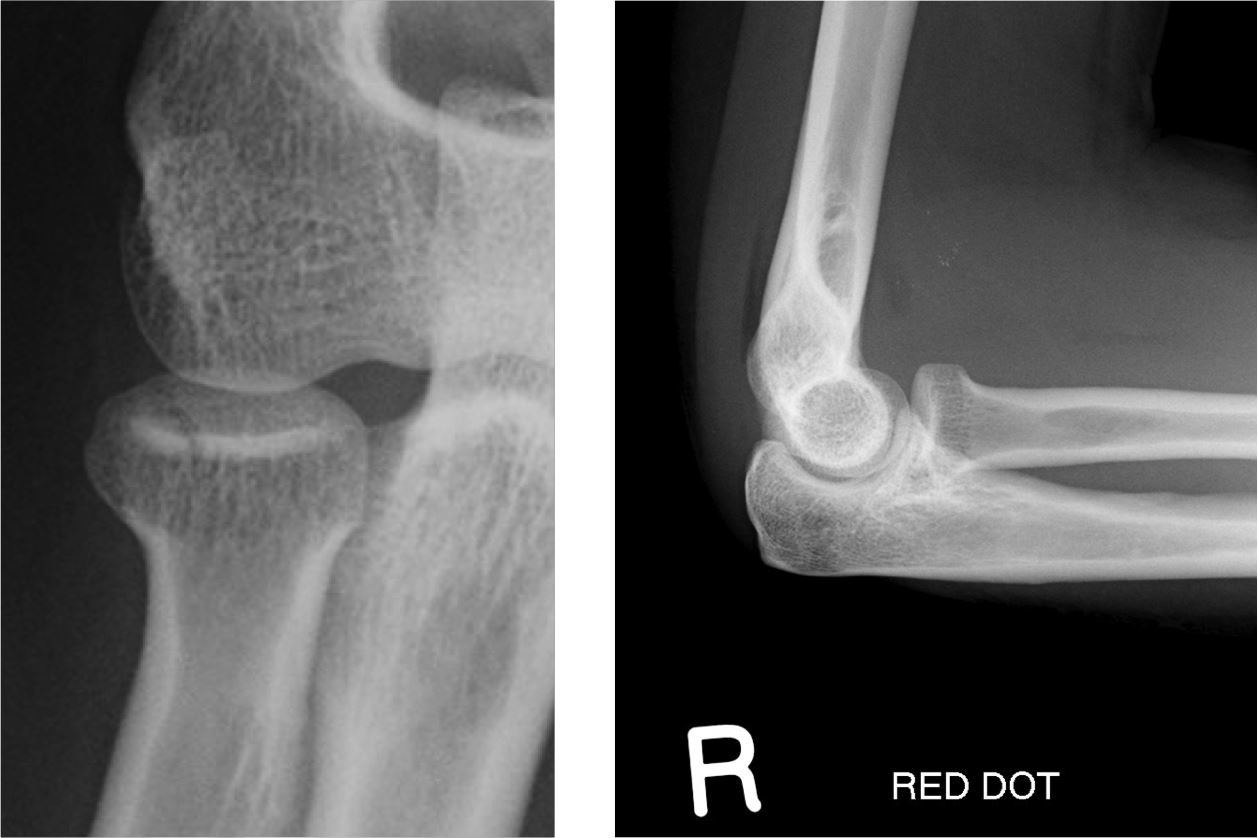
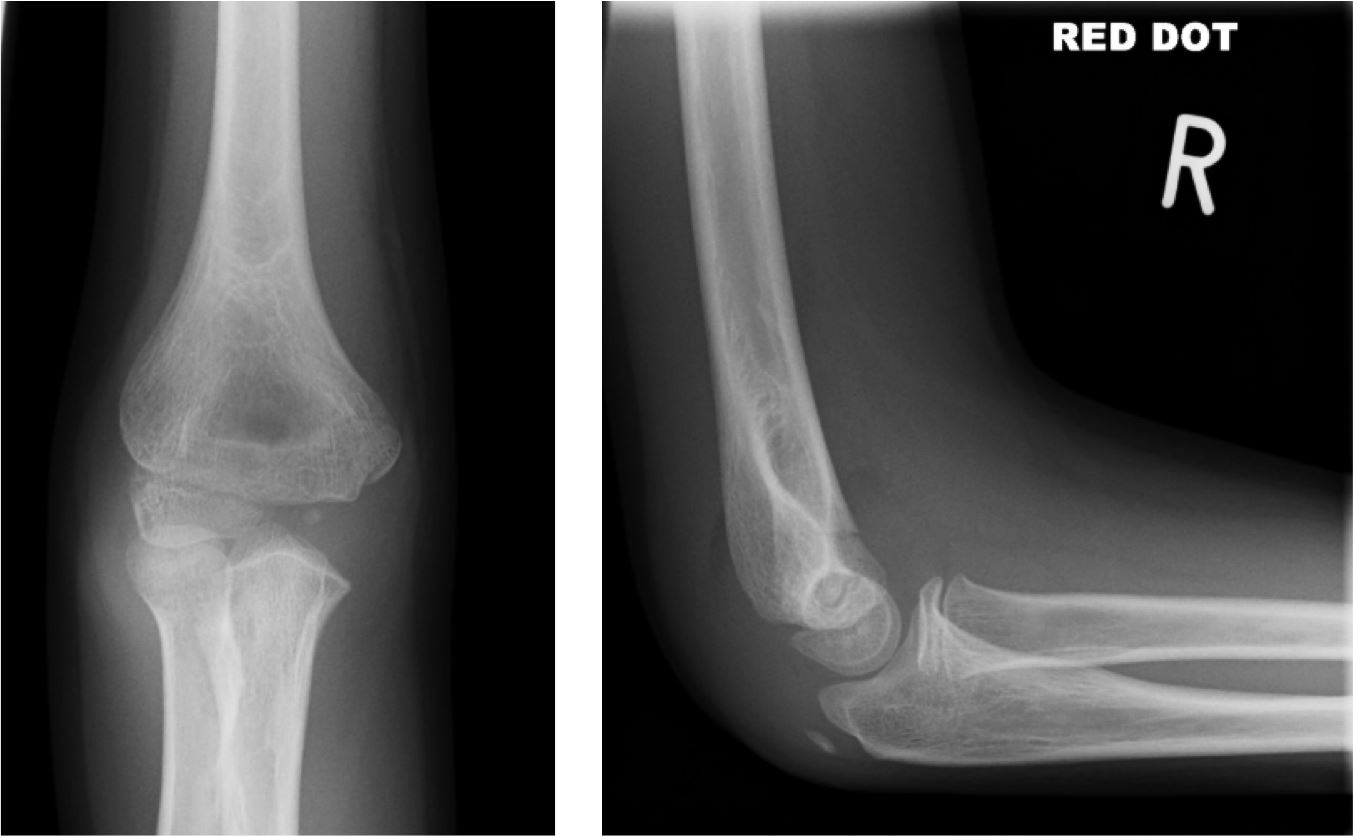
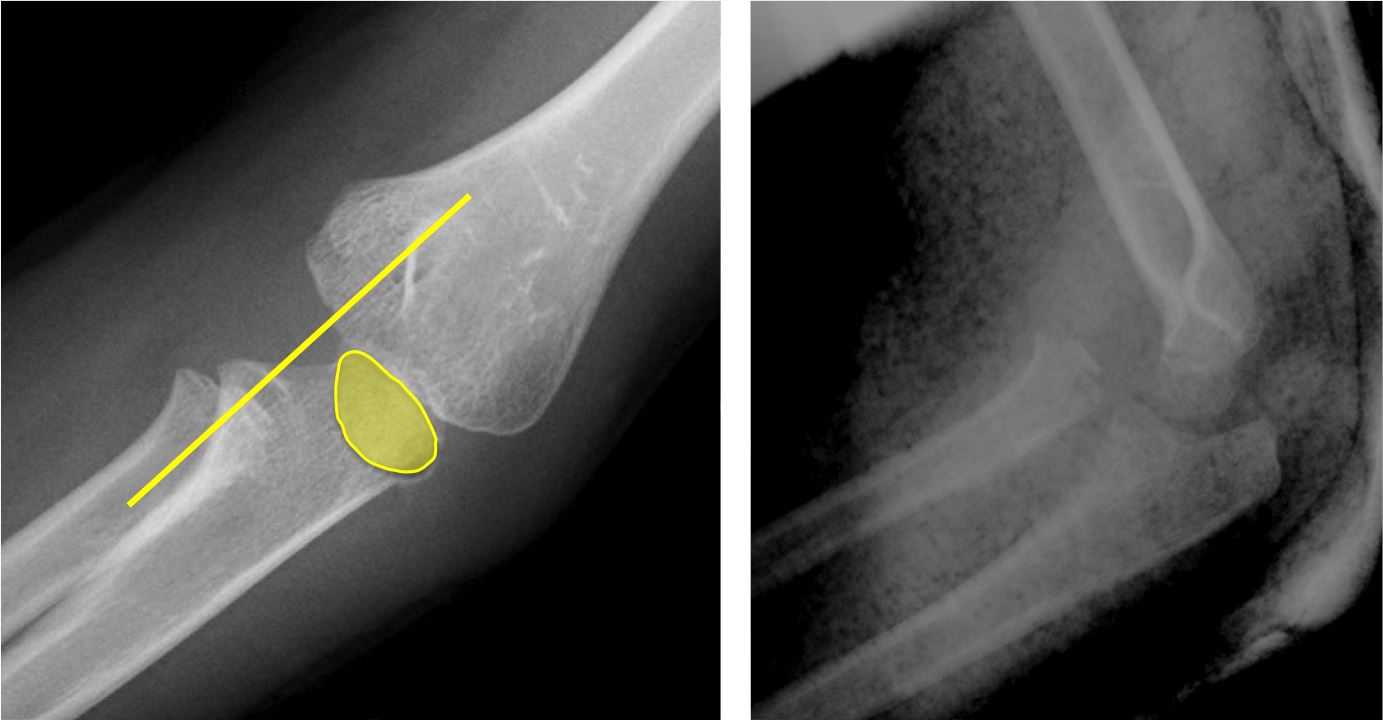
By far the most common type of fracture in adults. May be subtle; a positive fat pad sign may be the only evidence. Radial head/neck fractures may be visible as either:


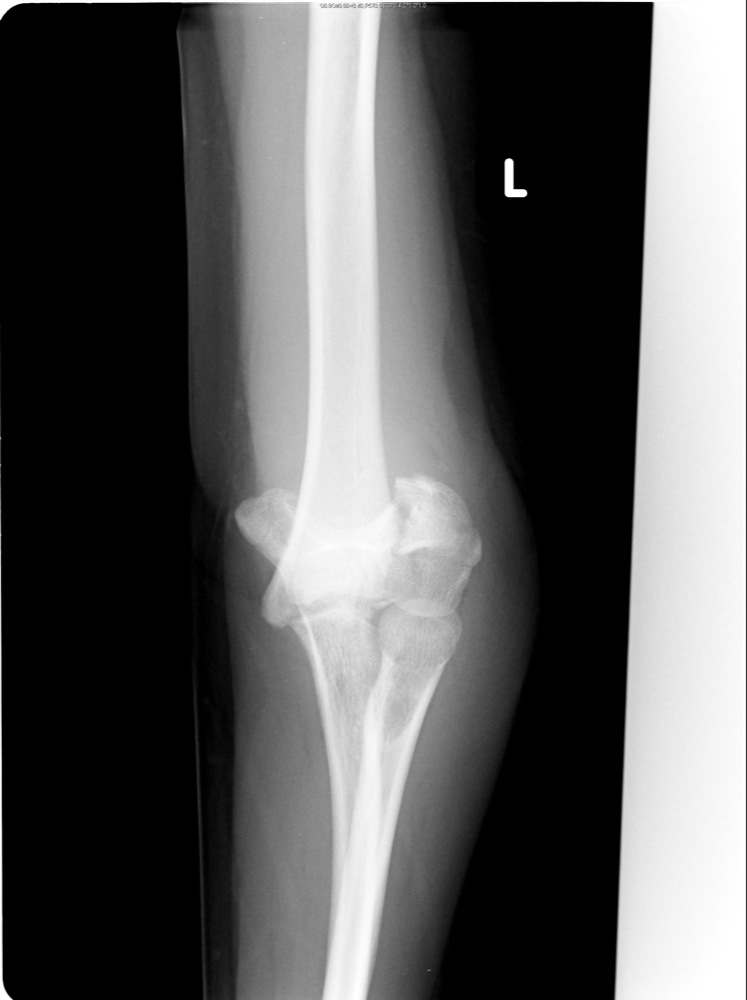




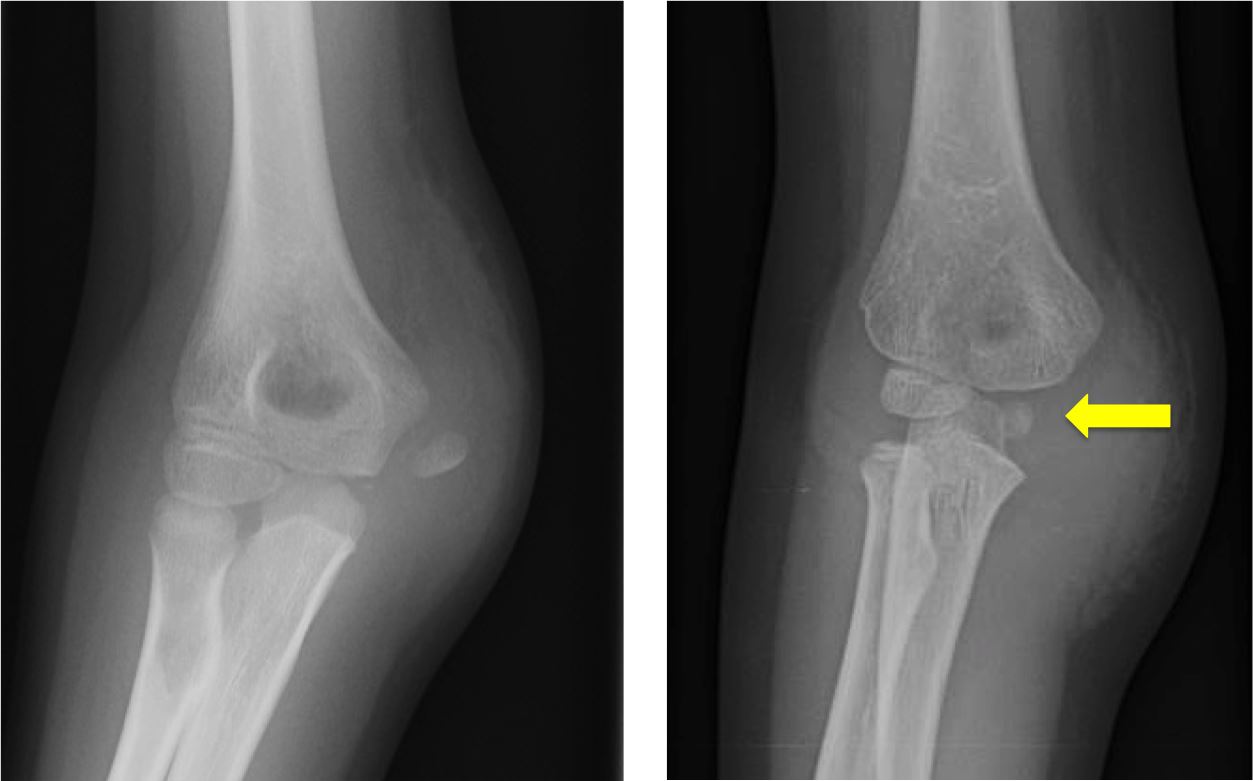
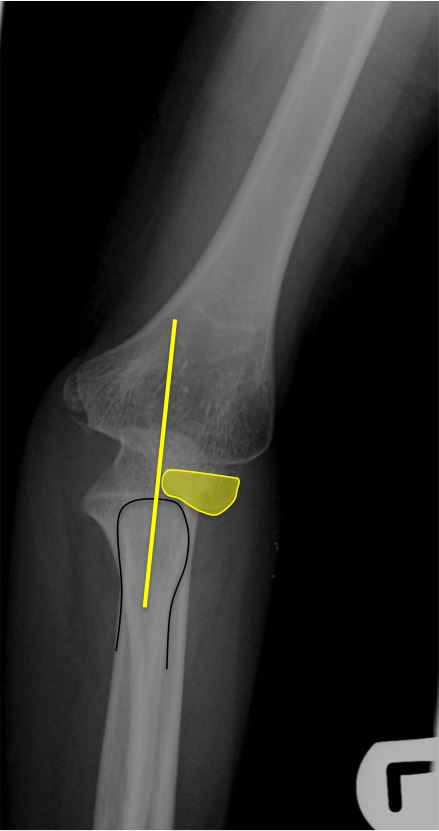
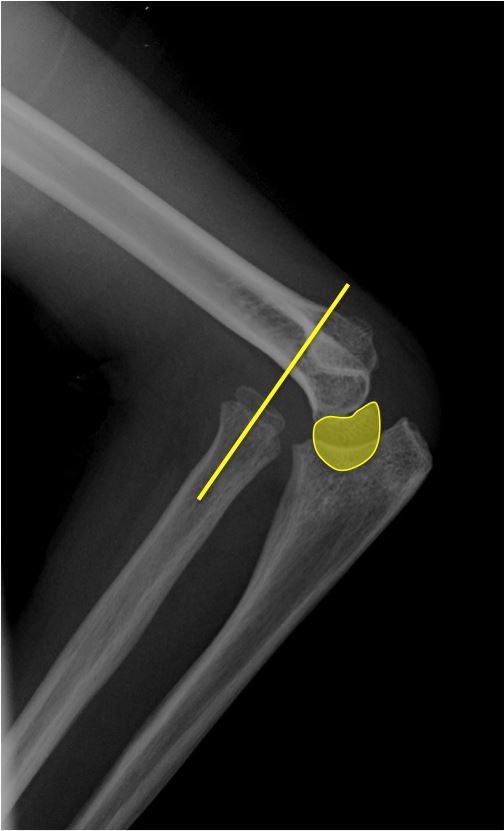
Treatment is simply supination of the forearm, which returns the ligament to its normal position. Radiography is not indicated.